We're excited about the impact donors can have by supporting our All Grants Fund and our Top Charities Fund. For donors who want to support the programs we're most confident in, we recommend the Top Charities Fund, which is allocated among our four top charities. For donors with a higher degree of trust in GiveWell and willingness to take on more risk, our top recommendation is the All Grants Fund, which goes to a wider range of opportunities and may have higher impact per dollar. Read more about the options for giving below. We estimate that donations to the programs we recommend can save a life for roughly $5,000 on average,[1] or have similarly strong impact by increasing incomes or preventing suffering. Click here to donate.
Why your support matters
We expect to find more outstanding giving opportunities than we can fully fund unless our community of supporters substantially increases its giving. Figures like $5,000 per life saved are rough estimates; while we spend thousands of hours on our cost-effectiveness analyses, they're still inherently uncertain. But the bottom line is that we think donors have the opportunity to do a huge amount of good by supporting the programs we recommend.
For a concrete sense of what a donation can do, let's focus briefly on seasonal malaria chemoprevention (SMC), which involves distributing preventive medication to young children. We've directed funding to Malaria Consortium to implement SMC in several countries, including Burkina Faso.[2]
In Burkina Faso, community health promoters go from household to household across the country, every month during the rainy season (when malaria is most common). They give medicine to each child under the age of five, which involves mixing a medicated tablet into water and then spoon-feeding the medicine to infants and having young children drink it from a cup. They also give caregivers instructions to give additional preventive medicine over the next two days.
It costs roughly $6 to reach a child with a full season's worth of SMC (though this figure doesn't account for fungibility, which pushes our estimate of overall cost-effectiveness downward).[3] If a child receives a full course of SMC, we estimate that they're about five times less likely to get malaria during the rainy season (which is when roughly 70% of cases occur).

Community distributor providing SMC medication to a child sitting on mother's lap. Photo courtesy of Malaria Consortium.
Imagine a village with 135 families in it, each with two kids under the age of five, for a total of 270 young children. In this village, imagine that every child is reached with a full course of SMC during the rainy season.[4] Without SMC, we estimate that on average, 100[5] of those 270 young kids would test positive for malaria at any given point in time (though we think most of them would be asymptomatic). We estimate that SMC brings the overall prevalence of malaria down from 100 kids to only 40.[6] For kids who would be symptomatic, this is the difference between feeling healthy and experiencing fever, aches, and other flu-like symptoms. And even more importantly: we estimate that SMC would protect one of these 270 young children from a fatal case of malaria.[7]
What we're excited to have recommended so far
This year, we've recommended grants to extend and expand programs we've supported for a while, like top charities, and we've also supported programs that are newer to us. With a decline in expected funding from Open Philanthropy, we've slowed our spending to match the funding we expect to raise going forward; we've focused more of our grantmaking on building for the future rather than funding large-scale opportunities this year. Below, we describe four selected grants from this year.[8]
More about each of these grants:
- $6.6 million to the Clinton Health Access Initiative (CHAI) to provide oral rehydration solution (ORS) and zinc for the treatment of diarrhea and to study the program's effectiveness. We've been interested in funding ORS/zinc for a long time; it appears to be a low-cost way to prevent and treat dehydration caused by diarrhea. Previously, we hadn't found the right opportunity to support it or to learn about our open questions. This grant will fund a randomized controlled trial studying the extent to which preemptively distributing free ORS/zinc directly to households increases usage by children under five, who are most at risk of death from diarrhea. This is the first program we've funded via the CHAI Incubator, a collaboration between GiveWell and CHAI designed to identify, assess, and scale highly cost-effective interventions.
- $12.6 million to New Incentives to extend and expand its promotion of infant immunization. New Incentives is one of our four top charities, which means it's one of the giving opportunities we're most confident in recommending to donors. With this funding, New Incentives is scaling up its work in northern Nigeria, where vaccination rates are particularly low and many children die of vaccine-preventable diseases. So far in 2023, New Incentives has enrolled over 1 million infants in its program.
- $5.8 million to MiracleFeet to scale up treatment for clubfoot and monitor its program. MiracleFeet's program is different from most of the programs we fund because it involves treating a physical disability rather than implementing a preventive health program. We currently estimate that this program is close to our cost-effectiveness threshold, and we hope that we'll learn more and update our views as a result of this work with MiracleFeet.
- $7.3 million to Evidence Action to explore opportunities to expand water chlorination and improve its effectiveness. This funding is intended to support Evidence Action to improve its safe water interventions and scope opportunities to expand to new settings. Evidence Action is also conducting pilots in three states in India; the goal is to explore the feasibility of different chlorination programs and partner with the government to deliver chlorination effectively.
What more donations will enable
With more funding, we can support more programs over the next few years. We research a variety of programs and estimate the cost-effectiveness of each, which varies by both program and location.
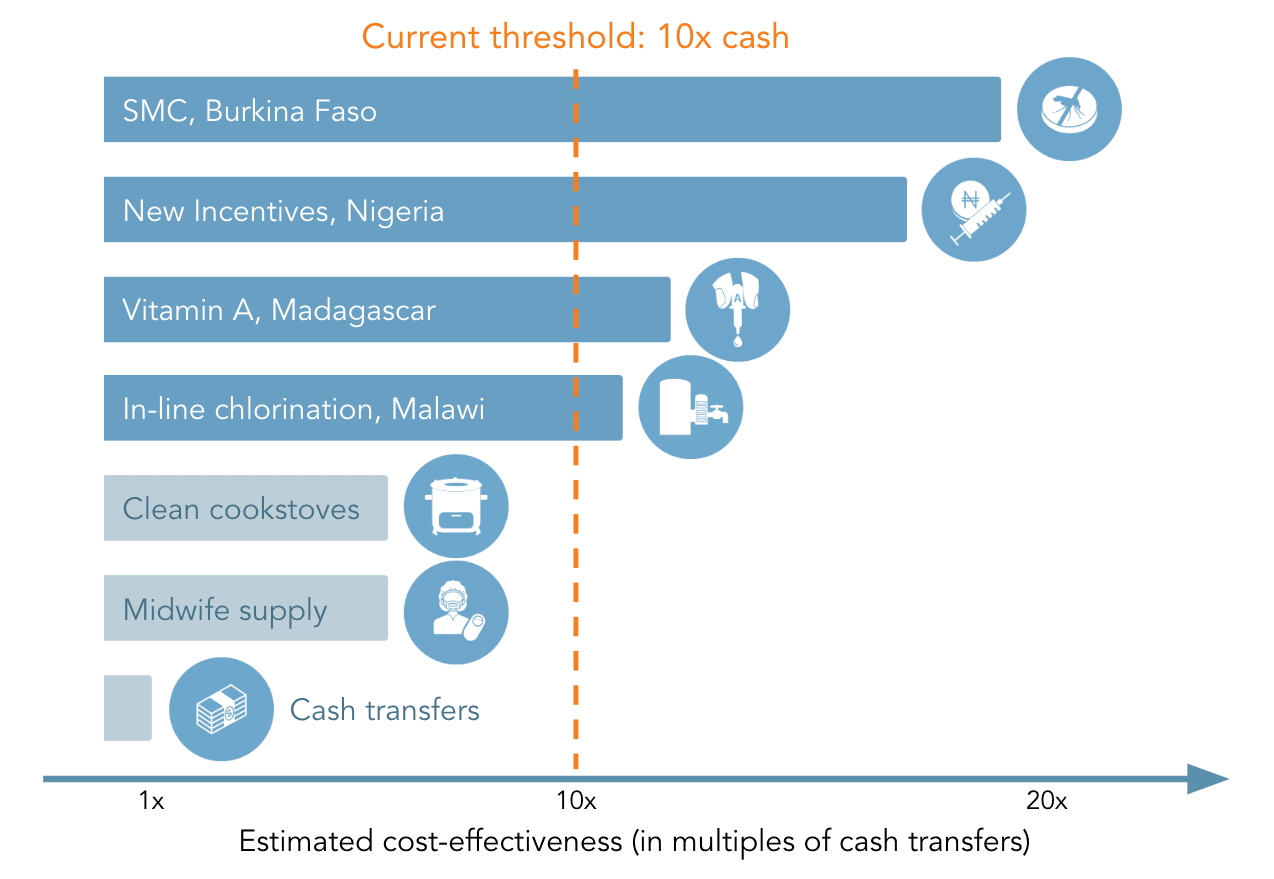
We set our cost-effectiveness threshold such that we expect to be able to fully fund all the opportunities above a given level of cost-effectiveness. Currently, we generally fund opportunities that we believe are at least 10 times as cost-effective as unconditional cash transfers to people living in poverty (i.e., "10x cash"). But there's nothing magical about the 10x cash threshold. We'd be very excited to recommend programs that are 6x cash, for example, if we had enough funding—a program that's 6x cash might save a life for less than $15,000.[9]
See below for a stylized representation of our cost-effectiveness threshold, with details in this footnote.[10]
If we had a very weak Giving Season this year and expected donations to continue lagging, we might have to raise our cost-effectiveness threshold to something like 12x cash and fund fewer programs going forward. In contrast, with exceptionally strong growth in donations we might be able to use a bar of 8x cash, expanding the set of opportunities we can fund.
Funding we receive this Giving Season could support a variety of programs at top charities and in areas that are newer to us; we're still in the process of researching those opportunities. A few examples of programs that we might support include:
- Iron fortification. When people consume iron-fortified wheat or rice, they're less likely to be iron deficient and anemic. In areas where iron deficiency is very common, we think fortification leads to cognitive benefits that also increase income and consumption.
- Malnutrition treatment. Children experiencing malnutrition are at higher risk of mortality. Severe acute malnutrition can be treated with ready-to-use therapeutic food and antibiotics. We wrote about malnutrition in 2021 and have continued to refine our analysis of malnutrition programs since then.
- Seasonal malaria chemoprevention (SMC). As discussed above, this program involves distributing preventive antimalarial medication to young children. We've directed about $400 million to Malaria Consortium for SMC throughout GiveWell's history.
- Vitamin A supplementation. Vitamin A deficiency prevents the immune system from functioning well, increasing the risk of death from infectious diseases. Twice-annual supplementation campaigns like Helen Keller International's reduce that risk.
How you can contribute
All Grants Fund
Our All Grants Fund is our top recommendation for donors who have a high level of trust in GiveWell and are open to programs that might be riskier than top charities.[11] It allows donors to contribute to the most impactful grant opportunities we’ve identified, regardless of program or location. When you give to the All Grants Fund, your donation might go to support research or scoping opportunities rather than straightforward delivery of programs. You can find examples of the types of grants that could be funded by the All Grants Fund here.
Top Charities Fund and specific top charities
If you want to give to the programs we have the highest confidence in, we recommend giving to the Top Charities Fund. The Top Charities Fund is allocated to the highest-priority funding gaps among our top charities only. Because it's more restricted, the Top Charities Fund may go to opportunities with lower expected value than the All Grants Fund; this would happen if our top charities become less funding-constrained than the rest of our portfolio, though so far we think the expected impact has been similar across the two funds. You can also give to a specific top charity of your choosing.
Unrestricted Fund
If you're open to supporting both GiveWell's operating expenses and our recommended programs, we recommend our Unrestricted Fund. If we raise more unrestricted funding than we need for our operating costs, we will grant out the excess. This is a great fit for donors who are excited about GiveWell's work and trust us to prioritize between our operations and our recommended programs.
You can read more about all options for making a donation here.
Your impact
Our community of donors will determine what we're able to fund in the future. By giving to any of the options above, you'll be supporting high-impact, evidence-backed programs. We're grateful for your contributions!
Notes
$5,000 is our conservative estimate of the impact of the average donation to one of our recommended life-saving programs (via top charities or the All Grants Fund). The estimated marginal cost to save a life (i.e., the cost-effectiveness of the "last" grant we make) is lower, around $7,500, but we think it generally makes sense for donors to think of the average in this context. We reached $5,000 by looking first at top charities, where the latest annual estimates range from $4,000 to $5,500 (rounded up to the nearest $500) by charity and more recent grants are in a similar range, as seen here. We then checked that $5,000 estimate against the life-saving grants we've recommended to non-top charities so far this year, and it seemed fair as a reasonable overall estimate. ↩︎
This example is of a top charity. The majority of the funding we direct goes to top charities, but we also fund programs beyond top charities, including research projects. Our top charities are all programs that prevent deaths primarily in young children, while some other programs we recommend primarily improve other health outcomes or increase incomes. ↩︎
This $6 figure doesn't account for other considerations, like whether another donor would have funded this program if GiveWell didn't. Those leverage and fungibility considerations mean we think that fewer than one additional child is reached per $6 donated, as some children may have received the medication in a world in which we didn't fund this distribution. ↩︎
In practice, it's unlikely that every child in a village would be reached with a full course of SMC. But, the $6 figure above refers to cost per child fully reached (setting aside fungibility), not just the cost per child targeted by the program. ↩︎
We calculate this by multiplying 270 children by a malaria prevalence of 37%, which results in 99.9 children testing positive for malaria. ↩︎
We calculate this by multiplying 270 children by the 22 percentage point reduction in malaria prevalence in the treated population, resulting in 59.4 children who would be protected by SMC, then subtracting that from the 99.9 likely to test positive for malaria: 99.9 - (270 * 22%) = 40.5. ↩︎
An estimate of 3.7 deaths averted per 1000 kids treated implies one death averted per (1000 / 3.7) = 270 kids treated. ↩︎
Estimated impact figures are based on our latest cost-effectiveness estimates, which are uncertain and could either overstate or understate actual impact. ↩︎
In our latest cost-effectiveness analysis, we estimate that New Incentives' program would be 6x cash in Yobe State, Nigeria, and cost $9,000 per life saved, and that the Against Malaria Foundation's long-lasting insecticide-treated nets program would be 5.5x cash in Chad and cost $14,000 per life saved. ↩︎
- This selection of programs is designed to be illustrative rather than representative of all our research. We caution against taking these estimates too literally, especially for the programs we aren't funding (where we've done limited work). Note also that 10x cash isn't a hard limit; we consider qualitative factors in our recommendations, as discussed here.
- More information about the programs in this chart, from top to bottom:
- Malaria Consortium's seasonal malaria chemoprevention program in Burkina Faso, estimated at 19x cash.
- New Incentives extension and expansion in northern Nigeria; grant recommended in May 2023. The cost-effectiveness of the grant will depend on how much funding goes to each state, with a lower-bound estimate of 17x cash.
- Helen Keller International's vitamin A supplementation program in Madagascar. Our estimate is that this program is about 12x cash, and we recommended funding it earlier this year.
- Evidence Action's in-line chlorination program in Malawi. We recommended a grant to this program in July 2022 and estimated it was around 11x cash.
- Clean cookstoves. We're very uncertain but estimate this to be very roughly 6x cash (though it could vary substantially, depending on the specific program and context).
- Programs to increase the supply of midwives. We're very uncertain but estimate this to be very roughly 6x cash (though it could vary substantially, depending on the specific program and context).
- Unconditional cash transfers, estimated (by definition) to be 1x cash. While we don't represent anything below 1x cash here, 1x cash isn't meant to represent the floor; we just focus our research on programs that we think are likely to be more cost-effective than cash.
After transaction fees, 100% of donations to the All Grants Fund are distributed to the recipient organizations. GiveWell does not use any of these funds for our own operating support. ↩︎