Arsenic: A toxicant worth thinking more about
This report summarizes a shallow investigation into the effects of arsenic on global health and wellbeing, interventions to reduce these effects, and existing programs in this space. I estimate that this report is the result of roughly 50 hours of research and writing. This report was produced as part of Cause Innovation Bootcamp’s fellowship program.
Edit 1/14/2022: Oscar Delaney points out that I misinterpreted a relevant piece of information, meaning that many of my estimates are off by a factor of ten. I have amended this piece to account for this error.
Summary
Arsenic is a toxicant that contaminates drinking water and other groundwater in some countries. This contamination typically results from groundwater flowing through soil and mineral deposits that contain arsenic in the right conditions to be soluble, but human activities can also lead to arsenic contamination in some cases.[1] [2] Approximately 300 million people live in areas where the groundwater is contaminated by arsenic to a degree that exceeds the World Health Organization Standard of 10 μg/L, and approximately 100 million of those people are exposed to arsenic levels in drinking water of more than 50 μg/L.[3] It is associated with a variety of negative health outcomes and other effects, resulting in higher mortality rates, cognitive damage, and lower lifetime incomes. Although Bangladesh has the most well-known and severe rate of arsenic contamination, groundwater arsenic affects many countries, and arsenic interventions outside of Bangladesh are relatively neglected. This report investigates various possible arsenic interventions. The lower bound for cost-per-death-averted was $6304; limiting only to interventions that are backed by field studies, the lower bound for cost-per-death-averted was $7749. Various factors, primarily uncertainty about the degree of harmful effects from arsenic, may reduce the overall cost-effectiveness, but arsenic interventions nonetheless have the potential to be promising, although at current margins they are likely less effective than Givewell top charities.
Introduction and Scope of the Problem
Human exposure to arsenic primarily results from groundwater contamination. Inorganic arsenic contamination in groundwater can lead to human exposure in three main ways: drinking contaminated water, using contaminated water for cooking, and using contaminated water to irrigate crops. The primary negative health effects of arsenic are increased risk of cancer and cardiovascular disease (including heart attacks), but other adverse effects include a higher risk of skin lesions, diabetes, pulmonary disease, stroke, cognitive deficits (in the case of prenatal and early childhood exposure), and (in some circumstances) Blackfoot disease.[4] [5] [6] [7] [8]
As of 2021, an estimated 300 million people worldwide live in areas with groundwater contaminated by arsenic (more than 10 μg/L), with approximately 100 million of those people living in areas with groundwater arsenic levels of more than 50 μg/L, which has been linked to an especially high likelihood of severe health consequences.[9] According to the World Health Organization, several countries have been found to have a high level of arsenic in groundwater, including Argentina, Bangladesh, Cambodia, Chile, China, India, Mexico, Pakistan, the United States of America, and Vietnam.[10] Arsenic exposure is particularly common in Bangladesh, where the number of people exposed to arsenic in groundwater has been estimated at 35 million - 77 million.[11] More recent estimates from 2012 indicate that remediation efforts have reduced this number to 19 million people exposed to arsenic levels greater than 50 μg/L,[12] and it is likely that this number has continued to decline since 2012.
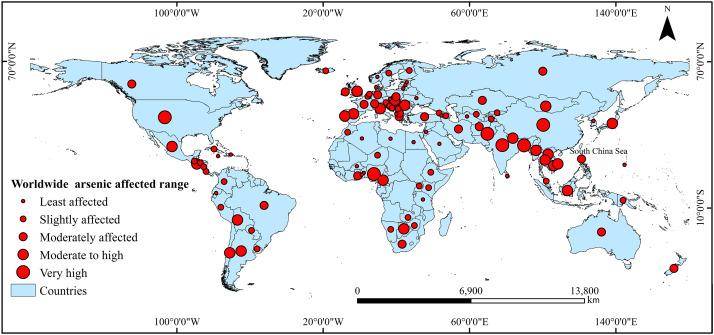
Arsenic contamination around the world.[13]
Various studies have attempted to determine the effects of arsenic exposure on overall mortality. A ten-year cohort study in Bangladesh[14] found that compared to people exposed to 0.1 - 10.0 μg/L of arsenic in well water, people exposed to 10.1–50.0 μg/L of arsenic in well water had an all-cause mortality rate 1.34 times higher (95% CI 0.99–1.82), people exposed to 50.1 - 150.0 μg/L of arsenic in well water had an all-cause mortality rate 1.09 times higher (95% CI 0.81–1.47), and people exposed to more than 150.0 μg/L (up to a maximum of 864.0 μg/L) had an all-cause mortality rate 1.68 times higher (95% CI 1.26–2.23). Although there is significant uncertainty in these numbers (in particular, several of the confidence intervals allow for the possibility that the mortality rate was the same or lower), the study estimated that in the cohort studied, 21.4% of all deaths in the population of people exposed to arsenic levels above 10 μg/L resulted from arsenic exposure. However, this study has been criticized for failing to account for differences in socioeconomic status by region, and may provide an overestimate of the true mortality difference. A 2004 study that considered only specific diseases that arsenic had previously been found to have a strong causal link with estimated that arsenic was responsible for a much smaller number of deaths -- 9,136 deaths and 174,174 DALYs per year, roughly 0.3% of the total disease burden in Bangladesh.[15] Another observational study, analyzing total mortality rates and mortality rates for a variety of diseases, found that the mortality rate for people who were exposed to high levels of arsenic was 1.32 times higher than the mortality rate for those who were not (95% confidence interval: 1.25 - 1.39).[16] However, this study focused on areas with extremely high rates of exposure, vastly exceeding even the 50 μg/L standard.
A 2011 review in Bangladesh estimated that in Bangladesh alone, arsenic exposure was responsible for 250,000 infant deaths per year and 200,000 - 300,000 cancer cases per "generation".[17] Although the number of infant deaths has likely decreased since then due to attempts at remediation, this serves to illustrate the approximate scope of the problem, particularly in areas that have not benefited from such remediation efforts. The same study referenced a rough order-of-magnitude estimate suggesting that exposure to 50 μg/L of arsenic increases cancer risk by 1 percentage point.
The number of contradictory findings makes it difficult to estimate the exact mortality burden of arsenic. The fact that arsenic primarily increases the risk of cancer and cardiovascular disease, which can take years to occur, also makes distinguishing between these possibilities more difficult. However, we can reasonably take arsenic being responsible for 0.3% of all deaths among those who were exposed to high levels of arsenic as a lower bound, and arsenic being responsible for 21.4% of deaths among those exposed as an upper bound. As these estimates are wildly divergent, they may result in significantly different cost-effectiveness numbers. (To be clear, both estimates have flaws making it unlikely that they are the “true value” -- but by taking them as a lower and upper bound, it is possible to get a sense of the cost-effectiveness of arsenic interventions under different assumptions.)
Arsenic has also been implicated as a likely cause of cognitive impairment[18], and reducing arsenic exposure levels could increase male incomes by up to 9% (although this is a maximum estimate, and therefore it likely overestimates the true value).[19] The typical proposed mechanism for the income effect is that arsenic leads to cognitive impairment and reduces the total amount of school completed, both of which reduce lifetime incomes.
Specifically with regards to arsenic in food, the mortality burden of arsenic in food has been estimated at 1.4 million DALYs/year from increased cancer risk and 49 DALYs/year from increased risk of coronary heart disease.[20] Arsenic contamination in food can result either from arsenic in water used to irrigate crops, or from arsenic in the soil used by crops itself. Unfortunately, many common methods of arsenic treatment will not affect this source of arsenic, but I have attempted to note exceptions.
Neglectedness
Various organizations and governments have attempted to remediate the negative effects of arsenic; an incomplete list can be found here.[21] However, so far, these interventions have mainly been focused on Bangladesh, due to the particularly high rates of arsenic poisoning in Bangladesh. Arsenic interventions outside of Bangladesh are comparably neglected, even in countries with significant levels of arsenic contamination, and could be high-impact.
Furthermore, interventions have been largely focused on digging deep tubewells.[22] This could be problematic both because of increases in deaths from pathogens and because of the mixed effectiveness of digging deeper wells.
Possible interventions and theory of change
Several possible interventions and the theory of change for each of them are listed below. The interventions are discussed in more detail, including effect size and cost-effectiveness estimates, in a later section.
| Intervention | Outputs | Outcomes | Quality of Evidence | Approximate cost-effectiveness | Overall promisingness |
| Adsorption of arsenic from water | Uncontaminated well-water (and possibly other water sources) | People can use clean drinking water for drinking and cooking | Moderate | High- lower bound of $7136-7749/death averted | High |
| Use ion exchange process to filter arsenic through a resin bed before drinking | Uncontaminated drinking water | People can use clean drinking water for drinking and cooking | Low | High- lower bound of $6304/death averted | Moderate |
| Dig deep tubewells that are not contaminated by arsenic to provide an alternative drinking water source | Uncontaminated drinking water | People can use clean drinking water for drinking and cooking | Moderate | Highly variable | Moderate/high variance |
| Testing water sources in areas with high arsenic contamination levels to determine which locations have greatest arsenic contamination | List of locations with the highest arsenic levels in water supplies | Interventions can be prioritized based on which areas have more severe arsenic contamination levels → Arsenic remediation programs can be implemented in the areas where they will have the most impact | Moderate | $4.79 - $5.32/test (not including distribution costs) | Moderate |
| Add membranes or other water filters at water pumps or in households to filter out arsenic | Uncontaminated or less contaminated water from pumps | People can use clean drinking water for drinking and cooking | High | High- lower bound of $173746/death averted | Low |
| Precipitate arsenic from well water by reacting it with other minerals to create solid compounds that are not water-soluble | Uncontaminated well water (and possibly other water sources) | People can use clean drinking water for drinking and cooking | Low | Unclear | Low |
| Treat arsenic-heavy soils with lime | Soil is not contaminated with arsenic, reducing contamination in wells | People can use clean drinking water for drinking and cooking. Crops are less contaminated. | Low | Unclear | Low |
| Treat drinking water with citrus | Uncontaminated drinking water | People can use clean drinking water for drinking and cooking | Moderate | Unclear | Low |
In general, these interventions can be roughly divided into three main categories: providing alternative sources of water, treating the existing sources of water, and collecting more data to improve intervention targeting. One important factor to keep in mind is that many of these interventions are easiest to target in wells, and may not be nearly as effective at reducing arsenic contamination from crops.
Other ideas that I considered but did not write a detailed theory of change for: paying people to move to areas without arsenic-contaminated water (high likelihood of negative second order effects and low feasibility due to disruptiveness of moving), cementation to remove arsenic from water (pilot studies have suggested that cementation only reduces arsenic levels in water to 2 mg/kg), distributing arsenic testing kits to individuals (even if you know your water is arsenic contaminated, this does not mean you can do anything about it, and it is likely more efficient to test water on a water-source basis since multiple families may get water from the same source), and various forms of incentivising industrial actors not to contaminate groundwater (although this can sometimes be a source of arsenic, preliminary investigations pointed to naturally occurring inorganic arsenic as a much larger factor).
I did some preliminary research into various interventions relating to the provision of new water sources that are not contaminated by arsenic; however, recent research has found that in cases where changing to a different water source requires more than 300 meters of additional travel, increased mortality as a result of diarrhea substantially outweighs any mortality benefits of avoiding arsenic contamination.[23]
Interventions in more detail
Adsorption
Adsorption refers to a process in which a chemical accumulates as a film on top of a liquid (or solid). For a summary of the use of the adsorption process in drinking water treatment, see here.[31]
A systematic review of the adsorption process found that the effectiveness varies substantially depending on what chemical is used. However, due to other contaminants in the water, it is often difficult to reduce arsenic to safe levels (although this also depends heavily on which chemical is used for adsorption).[32]
A few chemicals that seem particularly promising based on a preliminary analysis include:
- Laterite: A laboratory study in Argentina[33] found that effectiveness varied depending on the specific type of laterite used, but that Misiones laterite was 99% effective at removing arsenic. The laterite itself was found to have a negligible cost, but transportation costs were estimated at $43 per year in 2003 dollars for a household using 40 L/day, which using our (higher) estimates of per capita water use for consistency with other estimates is equivalent to a cost of $108.77 per person per year, and would potentially be even higher outside of Argentina (the location of the Misiones). A field study of a laterite-based adsorption filter found that regardless of the initial concentration of arsenic in the groundwater, the filter could reliably reduce arsenic concentrations to below 10 μg/L.[34] The same study estimated the cost as between $0.20 USD and $0.30 USD/m3 (in 2017 dollars), including transportation and labor costs associated with distribution. This is theoretically equivalent to an inflation-adjusted cost of at most $9.12/person/year. (The lower costs than the laboratory study are likely due in significant part to not using Misiones laterite in particular.)
- Ferruginous manganese ore: A laboratory study using water samples from West Bengal found that ferruginous manganese ore could reduce the concentration of arsenic by 98.5% to 99.8%, typically bringing it to below the limit of detection.[35] The same study found that this ore cost $50-56 USD (2002 dollars, not including distribution costs) per metric ton. The study used 2 grams of this ore per liter of water, indicating that (in inflation adjusted dollars, and using a rough approximation for distribution costs) it would cost approximately $8.40/person/year.
- A combination of NaHCO3, KMnO4, and FeCl3 was tested in an analysis that included both laboratory and field studies.[36] The field study found approximately 97-98% effectiveness at reducing arsenic levels, with final concentrations of arsenic between 3.69 and 7.58 μg/L. The same study estimated the cost as being $0.000158/L (2013 dollars). It is unclear if this includes distributional costs, so to be on the safe side, I have assumed it does not. This yields a final cost of approximately $8.77/person/year. Another laboratory study found that at concentrations resembling the typical concentration in contaminated wells, this method could reduce arsenic concentrations to below 1 μg/L, although the final concentration of arsenic was higher when the starting concentration was much higher.[37] The same study estimated the cost of this process at $0.326 USD/m3 (2018 dollars), suggesting an overall cost per person per year of roughly $19.34.
Ion Exchange
Ion exchange is a process in which dissolved ions of some substance are exchanged with ions of a different substance with the same charge. Arsenic removal depends substantially on the pH of the water and the length of time the removal happens for, however, this process can remove up to 99.2% of arsenic in water depending on pH.[38] However, the effectiveness of the ion exchange process depends on the other contaminants present in the water,[39] and has been found to be less effective in surface water compared to water that just has arsenic.[40] The quality of these studies are somewhat limited due to primarily studying the effectiveness of ion exchange in a lab, and not in “real world” scenarios, despite empirical evidence that it is less effective in real world scenarios.
The cost of ion-exchange systems has been estimated[41] at roughly $0.49/kilogallon (2014 dollars), including labor cost but not other distributional costs, although this estimate is primarily based on implementation in the United States and I think it is likely that non-chemical costs would vary significantly depending on the country. Taking this estimate at face value and applying the same heuristic for distribution costs that I used previously, I estimate the total costs of this method to be approximately $7.42/person/year. One important note about this method is that it does require electricity access.
New Tubewells
Digging deeper tubewells that would be less contaminated by arsenic is a commonly used strategy for reducing the levels of arsenic in drinking water.[46] However, it is unclear how effective this strategy is; one study found that the average arsenic levels in a sample of deep tubewells in Narail Sadar, Bangladesh, was still 42.59 μg (much lower than the average level in shallow tubewells of 91.33 μg, but still roughly four times the WHO limit).[47] Another study in Bangladesh, which measured arsenic levels in about 6,000 wells, found that deep tubewells were much less likely to have arsenic levels greater than 50 μg/liter (8% vs. 25-75%).[48] However, although the researchers did not provide exact information, it appears from looking at the provided graphs that many deep tubewells still had arsenic levels of more than 10 μg/L.
Another major drawback of this plan is the possibility of increasing mortality due to increasing the distance to safe water, which can in some cases significantly outweigh the beneficial effects of arsenic reduction.[49] [50] However, this could be mitigated by ensuring that new wells are dug in locations that enable all families to have a deep tubewell within 300 meters of their house, although such measures would increase the cost due to the higher number of wells that must be dug.
The total cost of installing these wells is roughly $1000 - $2000/well (including distributional costs).[51] The number of people who use each well varies substantially, although in order for these wells to not increase deaths from pathogens the number would likely need to be relatively small. Using a rough estimate of 10 people per drinking well, with tubewells typically lasting 10-40 years,[52] we find a cost per person-year of clean water of between $2.50 - $20.
Data Collection
One possible meta-intervention is to collect more data on the levels of arsenic in wells and other water sources outside of Bangladesh. Although there is substantial data on arsenic levels in wells in Bangladesh, there is not as much information on arsenic levels in individual wells outside of Bangladesh. This information could be used to better target arsenic-related interventions.
The cost of individual kits for testing wells has been estimated as being between $0.17 and $6.60 (2012 dollars), not including distribution costs.[53] This is equivalent to roughly $0.22 to $8.67 in current dollars. Unfortunately, the effectiveness of field testing kits has been called into question.[54] More recent analysis has found that the effectiveness of testing kits varies by the type of kit, but that two types of tests (Lamotte and Quick II) are both accurate and precise.[55] These tests cost $4.16/test and $4.62/test respectively (2020 dollars), which is equivalent to roughly $4.79 and $5.32 in 2022 dollars (not including distribution costs).
Membrane filters and other non-adsorption-based filters
This method of arsenic treatment includes a variety of different methods of filtering arsenic through some sort of filter designed to prevent arsenic from passing through. Filter effectiveness varies widely by the type of filter used. A review of the cost-effectiveness of different arsenic removal methods found that many types of filters (including ceramic filters, which have commonly been used in Bangladesh) did not actually filter out arsenic well enough to meet WHO standards, were extremely expensive, or both.[24] However, this does not rule out the possibility of other types of filters, which were not studied, being cost-effective.
TFC (thin film composite) membranes, a common type of membrane, appear to reduce arsenic concentrations to below 10 μg/L, with exact reduction varying by pressure, but roughly 96% reduction at 1 bar of pressure.[25] The same study found that they were more effective than UF membranes, another common membrane type. However, this was tested solely in a lab and may not properly generalize to real-world interventions. Another study measuring the effectiveness of several different types of membranes found that TFC membranes could be up to 99.8% effective.[26] Although it did not provide detailed cost information for individual membranes, this study also found that membrane filters cost between $1.41 and $3.72 per m3 of water in 2021 dollars (with exact prices depending on whether the membrane was a reverse osmosis membrane or nanofiltration membrane). This suggests the total cost of providing one person with clean water for a year could be up to $204.50 in today’s dollars.
Other types of nanofiltration membranes have been suggested as a promising intervention but do not seem to be sufficiently effective, as confirmed by a systematic review of different nanofiltration membranes.[27]
Some evidence also suggests that even when people are provided with filters, they do not actually use them.[28]
Precipitation
This technique refers to combining arsenic-contaminated water with other chemicals to transmute the arsenic into a solid compound, which can more easily be removed. The effectiveness varies depending on several factors, but in the best case scenario it can reduce arsenic levels to “below the level of detection,”[29] although this result is somewhat confusing since the data provided indicate that even in the best case scenario precipitation seems to only reduce arsenic levels to about 25 μg/L. However, this study has various issues making it more difficult to generalize, such as only examining much higher starting concentrations.
More recent studies have found that depending on the chemicals used to precipitate the arsenic, it is possible to reduce arsenic levels to below 10 μg/L.[30] However, these studies are somewhat limited in generalizability, as they find that effectiveness depends on the level of aluminum contaminants, which cause the effectiveness and necessary time to vary.
I was not able to find information on the typical costs for arsenic precipitation. Due to this fact, the relatively limited effectiveness of precipitation, and other information I found about drawbacks of this method, I think precipitation is likely to be less cost-effective and reliable than other methods.
Treating Soil with Lime
Treating arsenic-heavy soils with lime appears to substantially reduce the arsenic concentration in the soil, potentially as low as 1.4 mg/kg.[42] However, it is unclear what the effect of this on drinking water arsenic concentration is, as this amount is significantly more than the recommended value for water (although not all of it would actually get into the water). This method is notable because it could potentially significantly reduce the levels of arsenic in crops grown in this soil, but I was unable to find further details on the level of this effect.. I was unable to find estimates of the cost of this treatment method.
Treating Drinking Water with Citrus
Lime was discussed frequently in sources I reviewed, but it does not appear to have a very substantial effect size -- in an observational study of a water treatment plant, it was found to reduce arsenic levels from 36 μg/liter to 16 μg/liter,[43] which is still above the recommended safe amount. Similarly, an attempt to use lime as part of a SORAS process to remove arsenic in a laboratory from actual groundwater found that it was only about 63 - 70.2% effective at removing arsenic, with final concentrations between 50 and 120 μg/L.[44] Although these studies may have generated worse results due to relying on actual arsenic-contaminated groundwater rather than being conducted purely in laboratory conditions, this nonetheless suggests that lime treatment of drinking water is not very effective. A 2019 review that included this study estimated based on given prices and inflation rates that the total cost of treating 1m3 of water with lime was roughly $0.49 in 2019 USD, although this does not include distributional costs.[45] A very rough estimate for the cost of treating one person’s water for a year is therefore $28.56. Tomato juice, which was analyzed in the same study, was moderately more effective, achieving 90.2-97% removal rates, but it still resulted in arsenic levels of between 10 and 30 μg. The cost of treating 1 m3 of water with tomato juice was estimated at $0.65 in 2019 USD (again, not accounting for distributional costs), meaning that a very rough estimate of the cost of treating water with tomato for a year is therefore $37.88.
Notes on Cost-Effectiveness Estimates
General notes on cost-effectiveness
Many of the interventions described above rely on assumptions about the amount of water people use each year. A survey from 2006 found that on average, people in Bangladesh use 3.53 liters of water per day for drinking and 6.71 liters per day for cooking (with a 95% confidence interval of 3.45–3.61 L and 6.52–6.89 L respectively), or approximately 10.24 L in total.[56] This means that treating 1 m3 of water is equivalent to providing roughly 97 days of drinking and cooking water for a single person. For water treatment solutions that are implemented at the well, the actual number of days of safe water provided by treating 1 m3 of water could be up to about six times lower, as water is also used for other non-consumption purposes, which is often obtained from the same wells that water for drinking and cooking is obtained from. For the purpose of the cost-effectiveness analysis in this section I will conservatively assume that treating 1 m3 of water is equivalent to providing 15 days of clean water for a single person, and that treating 25 m3 of water is therefore sufficient to provide clean water to a single person for one year.[57]
For the purpose of these calculations, the cost of each intervention was doubled in situations where more accurate distributional costs were not available to account for distributional costs. However, this heuristic likely underestimates the distributional costs of otherwise-cheap interventions and overestimates the distributional costs of expensive interventions.
To account for inflation, an inflation calculator[58] was used to convert prices to 2022 dollars. However, this is an imperfect proxy due to the fact that inflation rates may vary by country.
Our cost-effectiveness analysis can be summarized in the following spreadsheet:

I did not calculate cost-effectiveness information for interventions with low or unclear effectiveness. In some cases (such as the lime and tomato treatments) these interventions were also relatively expensive, which combined with their low efficacy meant they were very unlikely to be cost effective.
In creating these estimates, I largely discounted the income effect of arsenic treatment. I do think that this effect could be significant, and should be considered in further research, but the evidence for the effect is weaker. (I am less confident in this, but I also suspect that if the health effects of arsenic are on the lower end of the plausible range, that this suggests that there was significant income confounding, which has been suggested as a likely mechanism for overestimates of the health effects. I would expect this to indicate that the income effects are also less significant/subject to the same confounders.)
Edit 1/14/2022: With the mortality effects (but not the income effects) being off by a factor of ten, the income effects of arsenic are relatively more important. Unfortunately, they are also much more uncertain, but I have attempted below to create a model that incorporates their effects.
Overall cost-effectiveness varied substantially depending on the assumptions made about the effect of arsenic on mortality. Under the most generous assumptions about arsenic impacts on mortality, arsenic exposure prevention was moderately less effective than GiveWell top charities. The lower bound for cost-per-death-averted was $6304; limiting only to interventions that are backed by field studies, the lower bound for cost-per-death-averted was $7749. (The true cost-effectiveness is likely somewhat lower due to imperfect targeting). However, making narrower assumptions about the impact of arsenic on mortality rate, the interventions became much less cost-effective (at minimum roughly $449,696/death averted).
Edit 1/14/2022: I also created a secondary model designed to account for income effects. This is obviously heavily dependent on assumptions about the relative moral weight of income increases vs. averting deaths. For the purpose of this model, I made the following assumptions:
- Increasing 200 people's income by 1% for one year is approximately as valuable as averting 1 DALY. (This is based on OpenPhilanthropy's model.)[59]
- Averting a death from arsenic is roughly equivalent to averting 30 DALYs. (This may be somewhat incorrect in either direction: many causes of arsenic-based mortality primarily affect older adults, but these include various conditions that can significantly impact quality of life prior to death).
- As a simplifying assumption, increasing one person's income by 9% as roughly 9x as valuable as increasing it by 1%. This is arguably slightly inaccurate due to the diminishing marginal utility of money.
- Gaining the full benefit of the income effect requires treating arsenic continuously over someone's life -- it is possible that the main cognitive and income-based harms occur in childhood, but targeting arsenic interventions towards exclusively children would be difficult to impossible. I approximate average lifespan at 73 years (the life expectancy at birth in Bangladesh in 2019)[60], although the true value may vary by country. I approximate income effects as affecting someone for roughly 50 years.
- As the income effect has only been studied at all in men, I do not incorporate potential benefits to women's income in my cost effectiveness analysis (which therefore means I may underestimate the income benefits).
I modelled three scenarios: one without any income benefits, one where arsenic remediation increases income by half of the measured effect (4.5%), and one where it increases income by the full measured effect (9%), though the last scenario is very optimistic. All these models can be found in the cost-effectiveness spreadsheet. In the 4.5% scenario, I estimate arsenic remediation as costing roughly $5,174.88 - $6360.50 per life-equivalent saved. In the 9% scenario, I estimate arsenic remediation as costing roughly $4,388.72 - $5394.22 per life-equivalent saved.
Next Questions/Further Steps
Some further questions that I expect to be particularly relevant to this research include:
- Can we narrow down the range of mortality-resulting-from-arsenic? Right now, the level of uncertainty is a major barrier in cost-effectiveness estimates.
- How significant are the practical barriers to using adsorption as a method of removing arsenic, beyond those outlined in this report? Are any of them serious enough to make it difficult or impossible to scale outside of small-scale trials?
- How difficult would it be to redirect resources from one arsenic intervention to another? (For example, could work that is currently being directed towards digging replacement shallow wells be used instead for other interventions?)
- How does the significant lag time on the effects of arsenic interventions affect the effectiveness of arsenic-related interventions?
- How robust is the evidence for arsenic-contamination-related income effects? How does this affect the cost-effectiveness of arsenic interventions?
Conclusion
Overall, the most promising intervention appears to be adsorption (with any of several chemicals as promising options -- most notably laterite and NaHCO3, KMnO4, and FeCl3, which stand out due to being supported by field studies). Ion-exchange systems stand out as a more speculative option that could be more cost effective but will likely face implementation challenges when applied outside of the laboratory. Membrane filters, precipitation, and treatment with lime and other citruses appear to be either ineffective or not cost effective, even under very generous assumptions. Digging deep tubewells is a common option that is likely actively harmful as implemented, although the implementation problems are not insurmountable.
I identified a lower bound for cost-per-death-averted of $6304, or $7749 when limiting only to interventions backed by field studies. After incorporating income effects, this could be up to $4,388.72 - $5394.22, but this requires very optimistic assumptions. On the current margins, this is slightly less effective than Givewell top charities. I believe it has the potential to be a promising intervention in the future (as current interventions hit diminishing margining returns or are otherwise obviated), but at current margins it would likely be better to direct resources elsewhere.
Acknowledgements
Akhil provided guidance and mentorship, as well as feedback on my first draft. Leonie Falk and Chris Smith also provided feedback. Karolina Soltys provided accountability support and motivation.
- ^
Nordstrom, D. Kirk. “Worldwide Occurrences of Arsenic in Ground Water.” Science 296, no. 5576 (2002): 2143–45. https://doi.org/10.1126/science.1072375.
- ^
Herath, I., Vithanage, M., Bundschuh, J. et al. Natural Arsenic in Global Groundwaters: Distribution and Geochemical Triggers for Mobilization. Curr Pollution Rep 2, 68–89 (2016).
- ^
Throughout this report, I have used the language “exposed to arsenic” or “exposed to [some specific level of arsenic]” to indicate that one’s primary source of drinking water is contaminated by that level of arsenic.
- ^
Moon, K., Guallar, E. & Navas-Acien, A. Arsenic Exposure and Cardiovascular Disease:An Updated Systematic Review. Curr Atheroscler Rep 14, 542–555 (2012). https://doi.org/10.1007/s11883-012-0280-x
- ^
“Arsenic in Drinking Water,” 1999. https://doi.org/10.17226/6444.
- ^
Chen Y, Graziano JH, Parvez F, Liu M, Slavkovich V, Kalra T, Argos M, Islam T, Ahmed A, Rakibuz-Zaman M, Hasan R, Sarwar G, Levy D, van Geen A, Ahsan H. Arsenic exposure from drinking water and mortality from cardiovascular disease in Bangladesh: prospective cohort study. BMJ. 2011 May 5;342:d2431. doi: 10.1136/bmj.d2431. PMID: 21546419; PMCID: PMC3088786.
- ^
Oberoi, Shilpi, Aaron Barchowsky, and Felicia Wu. “The Global Burden of Disease for Skin, Lung, and Bladder Cancer Caused by Arsenic in Food.” Cancer Epidemiology, Biomarkers & Prevention 23, no. 7 (2014): 1187–94. https://doi.org/10.1158/1055-9965.epi-13-1317.
- ^
Tseng, Chin-Hsiao, Choon-Khim Chong, Ching-Ping Tseng, and Jose A. Centeno. “Blackfoot Disease in Taiwan: Its Link with Inorganic Arsenic Exposure from Drinking Water.” Ambio 36, no. 1 (2007): 82–84. http://www.jstor.org/stable/4315790.
- ^
Kumar, A., Ali, M., Kumar, R. et al. Arsenic exposure in Indo Gangetic plains of Bihar causing increased cancer risk. Sci Rep 11, 2376 (2021). https://doi.org/10.1038/s41598-021-81579-9
- ^
“Arsenic.” World Health Organization, December 7, 2022. https://www.who.int/news-room/fact-sheets/detail/arsenic.
- ^
Naujokas MF, Anderson B, Ahsan H, Aposhian HV, Graziano JH, Thompson C, Suk WA. The broad scope of health effects from chronic arsenic exposure: update on a worldwide public health problem. Environ Health Perspect. 2013 Mar;121(3):295-302. doi: 10.1289/ehp.1205875. Epub 2013 Jan 3. PMID: 23458756; PMCID: PMC3621177. Note that this is actually citing a study from 2001.
- ^
Flanagan SV, Johnston RB, Zheng Y. Arsenic in tube well water in Bangladesh: health and economic impacts and implications for arsenic mitigation. Bull World Health Organ. 2012 Nov 1;90(11):839-46. doi: 10.2471/BLT.11.101253. Epub 2012 Sep 14. PMID: 23226896; PMCID: PMC3506399.
- ^
Shaji, E., M. Santosh, K.V. Sarath, Pranav Prakash, V. Deepchand, and B.V. Divya. “Arsenic Contamination of Groundwater: A Global Synopsis with Focus on the Indian Peninsula.” Geoscience Frontiers 12, no. 3 (2021): 101079. https://doi.org/10.1016/j.gsf.2020.08.015.
- ^
Argos, Maria, Tara Kalra, Paul J Rathouz, Yu Chen, Brandon Pierce, Faruque Parvez, Tariqul Islam, et al. “Arsenic Exposure from Drinking Water, and All-Cause and Chronic-Disease Mortalities in Bangladesh (Heals): A Prospective Cohort Study.” The Lancet 376, no. 9737 (2010): 252–58. https://doi.org/10.1016/s0140-6736(10)60481-3.
- ^
Lokuge KM, Smith W, Caldwell B, Dear K, Milton AH. The effect of arsenic mitigation interventions on disease burden in Bangladesh. Environ Health Perspect. 2004 Aug;112(11):1172-7. doi: 10.1289/ehp.6866.
- ^
Shih-Meng Tsai , Tsu-Nai Wang & Ying-Chin Ko (1999) Mortality for Certain Diseases in Areas with High Levels of Arsenic in Drinking Water, Archives of Environmental Health: An International Journal, 54:3, 186-193, DOI: 10.1080/00039899909602258
- ^
Yunus, Mohammad, Nazmul Sohel, Samar Kumar Hore, and Mahfuzar Rahman. “Arsenic Exposure and Adverse Health Effects: A Review of Recent Findings from Arsenic and Health Studies in MATLAB, Bangladesh.” The Kaohsiung Journal of Medical Sciences 27, no. 9 (2011): 371–76. https://doi.org/10.1016/j.kjms.2011.05.012.
- ^
Tyler CR, Allan AM. The Effects of Arsenic Exposure on Neurological and Cognitive Dysfunction in Human and Rodent Studies: A Review. Curr Environ Health Rep. 2014 Mar 21;1(2):132-147. doi: 10.1007/s40572-014-0012-1. PMID: 24860722; PMCID: PMC4026128.
- ^
Pitt, Mark M, Mark R Rosenzweig, and M Nazmul Hassan. “Identifying the Costs of a Public Health Success: Arsenic Well Water Contamination and Productivity in Bangladesh.” The Review of Economic Studies 88, no. 5 (2020): 2479–2526. https://doi.org/10.1093/restud/rdaa087.
- ^
Oberoi S, Devleesschauwer B, Gibb HJ, Barchowsky A. Global burden of cancer and coronary heart disease resulting from dietary exposure to arsenic, 2015. Environ Res. 2019 Apr;171:185-192. doi: 10.1016/j.envres.2019.01.025. Epub 2019 Jan 11. PMID: 30665120.
- ^
http://bicn.com/acic/resources/arsenic-on-the-www/orgs-projs.htm
- ^
https://news.climate.columbia.edu/2019/11/26/arsenic-deep-wells-bengal-basin/
- ^
https://www.hbs.edu/ris/Publication%20Files/BFGH_WaterInfrastructure2022_b5d9e7aa-7646-4949-b46c-136c8b5d2f2d.pdf
- ^
Shan, Yina, Praem Mehta, Duminda Perera, and Yurissa Yarela. “Cost and Efficiency of Arsenic Removal from Groundwater: A Review,” 2019. https://doi.org/10.53328/kmwt2129.
- ^
Bahmani P, Maleki A, Daraei H, Khamforoush M, Rezaee R, Gharibi F, Tkachev AG, Burakov AE, Agarwal S, Gupta VK. High-flux ultrafiltration membrane based on electrospun polyacrylonitrile nanofibrous scaffolds for arsenate removal from aqueous solutions. J Colloid Interface Sci. 2017 Nov 15;506:564-571. doi: 10.1016/j.jcis.2017.07.086. Epub 2017 Jul 24. PMID: 28759856.
- ^
Kundu, Sukanya, and Milan Kanti Naskar. “Perspective of Membrane Processes for the Removal of Arsenic from Water: An Overview.” Transactions of the Indian Ceramic Society 80, no. 1 (2021): 28–40. https://doi.org/10.1080/0371750x.2020.1864665.
- ^
Siddique TA, Dutta NK, Roy Choudhury N. Nanofiltration for Arsenic Removal: Challenges, Recent Developments, and Perspectives. Nanomaterials (Basel). 2020 Jul 6;10(7):1323. doi: 10.3390/nano10071323. PMID: 32640523; PMCID: PMC7407220.
- ^
Hossain, Mohammed, Shamsun N. Rahman, Prosun Bhattacharya, Gunnar Jacks, Ratnajit Saha, and Marina Rahman. “Sustainability of Arsenic Mitigation Interventions‒an Evaluation of Different Alternative Safe Drinking Water Options Provided in MATLAB, an Arsenic Hot Spot in Bangladesh.” Frontiers in Environmental Science 3 (2015). https://doi.org/10.3389/fenvs.2015.00030.
- ^
Nenov, V., Dimitrova, N., Dobrevsky, I. and Rands, D.G. (1992), Effective Precipitation of Arsenic from Aqueous Solution by Iron(III) Sulfate. Acta hydrochim. hydrobiol., 20: 14-17. https://doi.org/10.1002/aheh.19920200104
- ^
Mello, Jaime Wilson, Massimo Gasparon, and Juscimar Silva. “Effectiveness of Arsenic Co-Precipitation with Fe-Al Hydroxides for Treatment of Contaminated Water.” Revista Brasileira de Ciência do Solo 42 (2018). https://doi.org/10.1590/18069657rbcs20170261.
- ^
https://archive.unu.edu/env/Arsenic/Robins.pdf
- ^
Nicomel NR, Leus K, Folens K, Van Der Voort P, Du Laing G. Technologies for Arsenic Removal from Water: Current Status and Future Perspectives. Int J Environ Res Public Health. 2015 Dec 22;13(1):ijerph13010062. doi: 10.3390/ijerph13010062. PMID: 26703687; PMCID: PMC4730453.
- ^
Bundschuh, Jochen, Prosun Bhattacharya, Ondra Sracek, M. Fernanda Mellano, Antonio E. Ramírez, Angel del Storniolo, Raúl A. Martín, Julia Cortés, Marta I. Litter, and Jiin-Shuh Jean. “Arsenic Removal from Groundwater of the Chaco-Pampean Plain (Argentina) Using Natural Geological Materials as Adsorbents.” Journal of Environmental Science and Health, Part A 46, no. 11 (2011): 1297–1310. https://doi.org/10.1080/10934529.2011.598838.
- ^
Mondal, Sourav, Anirban Roy, Raka Mukherjee, Mrinmoy Mondal, Sankha Karmakar, Somak Chatterjee, Munmun Mukherjee, Saikat Bhattacharjee, and Sirshendu De. “A Socio-Economic Study along with Impact Assessment for Laterite Based Technology Demonstration for Arsenic Mitigation.” Science of The Total Environment 583 (2017): 142–52. https://doi.org/10.1016/j.scitotenv.2017.01.042.
- ^
Chakravarty, S, V Dureja, G Bhattacharyya, S Maity, and S Bhattacharjee. “Removal of Arsenic from Groundwater Using Low Cost Ferruginous Manganese Ore.” Water Research 36, no. 3 (2002): 625–32. https://doi.org/10.1016/s0043-1354(01)00234-2.
- ^
Bordoloi, Shreemoyee, Suresh K. Nath, Sweety Gogoi, and Robin K. Dutta. “Arsenic and Iron Removal from Groundwater by Oxidation–Coagulation at Optimized Ph: Laboratory and Field Studies.” Journal of Hazardous Materials 260 (2013): 618–26. https://doi.org/10.1016/j.jhazmat.2013.06.017.
- ^
Bora, Anup J., Rajkamal Mohan, and Robin K. Dutta. “Simultaneous Removal of Arsenic, Iron and Manganese from Groundwater by Oxidation-Coagulation-Adsorption at Optimized Ph.” Water Supply 18, no. 1 (2017): 60–70. https://doi.org/10.2166/ws.2017.092.
- ^
Barakat, M.A., and S. Ismat-Shah. “Utilization of Anion Exchange Resin Spectra/Gel for Separation of Arsenic from Water.” Arabian Journal of Chemistry 6, no. 3 (2013): 307–11. https://doi.org/10.1016/j.arabjc.2010.10.011.
- ^
Agostina Chiavola, Emilio D'Amato, Renato Gavasci, Piero Sirini; Arsenic removal from groundwater by ion exchange and adsorption processes: comparison of two different materials. Water Supply 1 October 2015; 15 (5): 981–989. doi: https://doi.org/10.2166/ws.2015.054
- ^
Karakurt S (2019). Removal of Carcinogenic Arsenic from Drinking Water By the Application of Ion Exchange Resins. Oncogen 2(1): 5.
- ^
Sorg, Thomas J., Lili Wang, and Abraham S. Chen. “The Costs of Small Drinking Water Systems Removing Arsenic from Groundwater.” Journal of Water Supply: Research and Technology-Aqua 64, no. 3 (2014): 219–34. https://doi.org/10.2166/aqua.2014.044.
- ^
MOON, D, D DERMATAS, and N MENOUNOU. “Arsenic Immobilization by Calcium–Arsenic Precipitates in Lime Treated Soils.” Science of The Total Environment 330, no. 1-3 (2004): 171–85. https://doi.org/10.1016/j.scitotenv.2004.03.016.
- ^
Fields, K., A. Chen, AND L. Wang. ARSENIC REMOVAL FROM DRINKING WATER BY COAGULATION/FILTRATION AND LIME SOFTENING PLANTS. U.S. Environmental Protection Agency, Washington, D.C., EPA/600/R-00/063 (NTIS PB2001-100152), 2000.
- ^
Majumder, Santanu, Bibhash Nath, Simita Sarkar, Sk. Mijanul Islam, Jochen Bundschuh, Debashis Chatterjee, and Manuela Hidalgo. “Application of Natural Citric Acid Sources and Their Role on Arsenic Removal from Drinking Water: A Green Chemistry Approach.” Journal of Hazardous Materials 262 (2013): 1167–75. https://doi.org/10.1016/j.jhazmat.2012.09.007.
- ^
Shan, Yina, Praem Mehta, Duminda Perera, and Yurissa Yarela. “Cost and Efficiency of Arsenic Removal from Groundwater: A Review,” 2019. https://doi.org/10.53328/kmwt2129.
- ^
https://www.chemistryworld.com/features/digging-deep-for-safer-water/7218.article
- ^
Mohana, A. A., Md. A. Rahman, and Md. R. Islam. “Deep and Shallow Tubewell Water from an Arsenic-Contaminated Area in Rural Bangladesh: Risk-Based Status.” International Journal of Energy and Water Resources 4, no. 2 (2020): 163–79. https://doi.org/10.1007/s42108-020-00059-4.
- ^
van Geen, A., Y. Zheng, R. Versteeg, M. Stute, A. Horneman, R. Dhar, M. Steckler, et al. “Spatial Variability of Arsenic in 6000 Tube Wells in a 25 Km2Area of Bangladesh.” Water Resources Research 39, no. 5 (2003). https://doi.org/10.1029/2002wr001617.
- ^
https://www.hbs.edu/ris/Publication%20Files/BFGH_WaterInfrastructure2022_b5d9e7aa-7646-4949-b46c-136c8b5d2f2d.pdf
- ^
Goel V, Islam MS, Yunus M, Ali MT, Khan AF, Alam N, Faruque ASG, Bell G, Sobsey M, Emch M. Deep tubewell microbial water quality and access in arsenic mitigation programs in rural Bangladesh. Sci Total Environ. 2019 Apr 1;659:1577-1584. doi: 10.1016/j.scitotenv.2018.12.341. Epub 2018 Dec 24. PMID: 31096367; PMCID: PMC6724724.
- ^
https://www.chemistryworld.com/features/digging-deep-for-safer-water/7218.article
- ^
Afzal, Mohammad. “STATISTICAL ESTIMATION OF USEFUL LIFE OF TUBEWELLS.” The Pakistan Development Review 12, no. 1 (1973): 81–90. http://www.jstor.org/stable/41258184.
- ^
George, Christine Marie, Yan Zheng, Joseph H. Graziano, Shahriar Bin Rasul, Zakir Hossain, and Alexander van Geen. “Evaluation of an Arsenic Test Kit for Rapid Well Screening in Bangladesh.” Environmental Science & Technology 46, no. 20 (2012): 11213–19. https://doi.org/10.1021/es300253p.
- ^
Rahman, Mohammad Mahmudur, Debapriyo Mukherjee, Mrinal Kumar Sengupta, Uttam Kumar Chowdhury, Dilip Lodh, Chitta Ranjan Chanda, Shibtosh Roy, et al. “Effectiveness and Reliability of Arsenic Field Testing Kits: Are the Million Dollar Screening Projects Effective or Not?” Environmental Science & Technology 36, no. 24 (2002): 5385–94. https://doi.org/10.1021/es020591o.
- ^
Reddy, Raghav R., Grace D. Rodriguez, Tara M. Webster, Md. Joynul Abedin, Md. Rezaul Karim, Lutgarde Raskin, and Kim F. Hayes. “Evaluation of Arsenic Field Test Kits for Drinking Water: Recommendations for Improvement and Implications for Arsenic Affected Regions Such as Bangladesh.” Water Research 170 (2020): 115325. https://doi.org/10.1016/j.watres.2019.115325.
- ^
Milton, Abul Hasnat, Habibur Rahman, Wayne Smith, Rupendra Shrestha, and Keith Dear. “Water Consumption Patterns in Rural Bangladesh: Are We Underestimating Total Arsenic Load?” Journal of Water and Health 4, no. 4 (2006): 431–36. https://doi.org/10.2166/wh.2006.0027.
- ^
1000 L/62.47 L consumed per day from all sources (including non tubewell sources), rounded down to account for potential uncertainty.
- ^
https://www.usinflationcalculator.com/
- ^
https://www.openphilanthropy.org/research/technical-updates-to-our-global-health-and-wellbeing-cause-prioritization-framework/
- ^
https://data.worldbank.org/indicator/SP.DYN.LE00.IN?locations=BD
- ^
https://pip.worldbank.org/country-profiles/BGD
Hi Francis, thanks for this thoughtful write-up, I didn't realise so many people were exposed to dangerous levels of arsenic!
I have some (perhaps) sad news though, that I believe your cost-effectiveness estimates are 10x too optimistic: you list the annual mortality rate in Bangladesh as 5.5%, however the source you cite gives the (far more plausible - 5% would imply a life-expectancy on the order of 20) figure of 5.5 per thousand.
This, combined with the fact that I basically buy your/others' critique of Argos 2010 that not taking into account socioeconomic differences makes the correlational analysis not very informative, makes me think the bottom line is arsenic interventions are very likely not on the same order of cost-effectiveness as GiveWell top charities.
Given the above, perhaps this is a moot point, but I am interested in adsorption because you say it is the best intervention. I think it would be useful to say something about the practicalities of the process. Is it as simple as dropping a bag of chemicals into a well and letting chemistry happen? It feels important to me to know how simple (and hence scalable) the intervention is.
Finally, two suggestions on communication:
Thanks Oscar! I really appreciate you catching that. I've revised the post to reflect the more accurate statistics.
With regards to your question, the sources I found seemed to mostly describe adsorption as a relatively simple process -- e.g. Nicomel et. al. specifically highlighted "easy operation and handling" as a major advantage of adsorption (and gave that as a reason for why it has been commonly used in the past).
OK nice, thanks for the prompt changes, especially the new income effects part of the model!