September 1, 2021 update:
DMI does not have data on the effects of mask wearing in reduction COVID-19 incidence or DALY burden, however, it refers to the $7-27 per DALY cost of a COVID-unrelated radio-based behavior change campaign. Thus, this program could have been more or less cost-effective than that of DMI.
However, it could have been done much better (targeting healthcare providers or community leaders with generous mask cash advance (to be used per discretion and masks made e. g. of local material) and role model expectations/accountability and perhaps the poster).
Also, the war may be a much more significant contributor to DALY burden (both in terms of health-related quality of life (HRQoL) and deaths), so, spending the $3,600 to pay e. g. 5 local university graduates to each work full-time for 9 weeks ($2/hour or $8/day) on developing and advancing solutions and managing them/asking questions and brainstorming solutions with the skilled volunteer work could have been a better philanthropic investment.
So, potentially, a cost-effective solution is that skilled decisionmakers obtain information on fundamental local problems and work with underemployed locals (to allow for lower wages and perhaps gain more sincere/locally understanding thoughts) to resolve these issues. Outcomes can be measured by a single metric, such as improvements in HRQoL.
August 30, 2021 update
Please correct any mistakes.
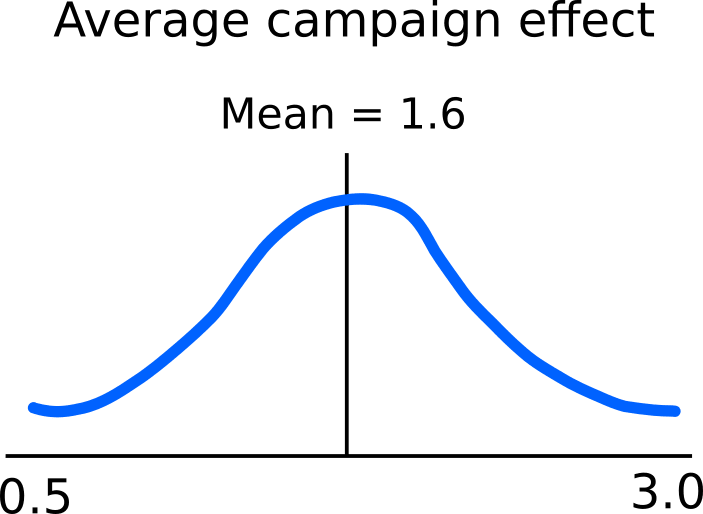
Effects on mask wearing
The before and after data has been analyzed. As per the analyst, “Preliminary findings: The mean effect on mask-wearing is an increase of about 1.6 in the log-odds ratio (very roughly equivalent to a 300% increase in mask-wearing) -- 94% credible interval is (1.1, 2.1). … The absolute increase in mask wearing was somewhere around 5 percentage points.”
Using a very simple [after-before(program) - after-before(control)] analysis in Sheets, the increase in mask wearing is 8 percentage points. This may be reasonable, since the analyst used weak priors.
[Visualization of a graph, titled "% Mask wearing" that shows Before and After situation for Control (1.6% to 3.4%) and Program (from 0.8% to 11.4%). "8.8 pp attributable to program is shown by a vertical arrow on the right (at After)."]
Using a linear regression (R code for Bayesian and linear regressions here),
maskCount = a1campaign*followup + a2log_pop + a3log_pop*followup + a4date,
the increase attributable to the program is about 8.82 percentage points (a1=48.5, which is the number of masks out of 550 that the fact that the community is campaign and is observed after the program, at followup. (48.5/550)*100=8.82).
Thus, we deduce that
[after-before(program) - after-before(control)]
calculations in Sheets can estimate effects attributable to the program (assuming program and control comparability and study units comparability to the general population) with an error of a factor of about 2.
Costs
The total cost of this program was $3,650. This comprised of:
- Volunteer stipend (in-person through-networks informing groups) (34 volunteers (6 teams), total of 0.9 FTE (about 1,800 hours)): $1,520
- Radio show: $1,280
- Newspaper articles: $520
- Flyers posted at central locations in community: $200
- Transportation: $100
- Miscellaneous: $30
Cost-effectiveness
The total population of the campaign communities is approximately: 25,100.
That is $3,650/25,100 = $0.145 to quadruple one’s chance to wear a mask or to increase it by 5 percentage points (conservative estimate).
We are not sure about the cost-effectiveness of this project compared to that of DMI’s COVID programming, however, we are asking DMI. We will also appreciate assistance in estimating cost-effectiveness in terms of $/QALY or $/case averted, in case you can share with us any epidemiological insights.
Cost-effectiveness of the program approach compared to targeting healthcare providers
Potentially, the program’s cost-effectiveness could have been increased. Low percentage of healthcare providers (about 5%) wore masks. Providing them with a stipend to purchase masks (alongside with local networks’ expectations and accountability) and a poster to inform patients about the preventive standards and their importance could have increased the normalization of preventive measures more effectively. However, it is unclear whether some remote communities would have gathered this information (according to this program, as of November 2020, no primary healthcare facilities operate in many villages).
Cost-effectiveness of the program approach in the local context
In addition, other programs could have been prioritized in order to benefit the community optimally. Further data is needed to estimate the wellbeing effects of reduced COVID risk given the ongoing war. For example, an increasing mortality due to COVID (with limited assistance due to government clinic closures and low NGO presence) could have made a barely-worth-living situation negative. Or, coronavirus could have not affected the health situation substantially (patients die commonly due to missing funds) and skilled work could have been better utilized to improve local institutions’ decisions (mitigate the conflict), which could be the necessary and sufficient determinant of persons’ increased wellbeing. Or, skilled work could have been used to improve the global governance system that leads some groups to be resolving perceived issues through armed conflict. (This program has not developed connections with local rebel leaders. Relatedly, the Reach Out Cameroon project has but ended in November 2020.)
[Imagine this image from the region with "masks but war" on it.]
Learnings
Learnings from this project include:
- Expecting an organizer to keep funds while waiting for evidence in low resource settings may constitute an unnecessary issue. The volunteers and locals were given about $1,040 as need-targeted cash transfers. This could have been still allocated cost-effectively, since the organizer presented an authority and local networks accountability in one approaching the decisionmaker only in great need and somewhat as a last resort (high counterfactual impact).
- In this case, distance (as well as community standards (no personal gain) or a locally vetted life-threatening personal needs fund when considering EAs from low resource settings – to what extent their networks?) can be used as a sufficient shield from local immediate needs that could bias resource allocation (if every day, only 10 close neighbors asked for only $10 to cover a medical expense, or to feed a hungry child, in a month, the COVID prevention budget would have been used). For instance, allocation decisions can be made internationally (or across moral circles or just rationally), through understanding local priorities and aiming to uncover reasoning biases. Subsequently, budgets can be provided only for the highest priorities.
[Imagine this image with a red circle with a line across it over it.]
- Relatedly, contractors paid a limited amount (e. g. > $1/hour) may benefit from an ‘emergency’ fund for immediate needs (in lieu of a higher hourly stipend). For example, volunteers can be paid the minimum wage (or assist in their communities unpaid) but for every number of hours be eligible for a need-based one-time assistance. Then, volunteers can feel cared for in need (which a sample of 30 respondents in a slum would give up 78% of their remaining life for (q13)), prevent any perception of burden (rejection of many/all close ones before finding a sponsor when in dire need may lead to low wellbeing of entire networks), and encourage skill development for the purpose of sharing (persons being transparently preferred in assistance due to their own help).
[This image with a note that minimum wage + bonus = 100-200% of the minimum wage and a happy green smile.]
- Persons in low resource settings may confuse Effective Altruism with ‘we understand, care, and can help specifically you with your hardships.’ Either, it can be explained that their issues are not as cost-effective to address, or if they are, there is just an extensive room for skills and funding and it does not matter who is helped, so why not someone else or that if cost-effective measures are locally identified, then also sustainable local sourcing should be developed or if that is not possible then the problem should be addressed otherwise (such as by increasing personal capacity to think of and test innovative solutions, e. g. through participating in EA) – or just preventing the confusion by working with an NGO that is clear in only having funds for this program (then, persons will not participate in EA or develop innovative solutions). Thus, possibly, emphasizing the standard of no personal gain but an opportunity to develop and share skills/cost-effective solutions for free (while potentially gaining perks such as support in helping more) can prevent suboptimal appeals (e. g. to buy more nutritious meals which can be extremely cost-ineffective) and discourage/exclude persons who may seek dependency on a resourceful network.
[Imagine the words "Personal gain" with the red circle with a line across its diameter under it.]
- Persons with high relevant capital (e. g. ability to influence local networks to change their behaviors based on understanding a topic) can be hired for low wage (e. g. here, $0.85/hour including all emergency community bonuses).
[Imagine the words "Dream team" on an image with two sprocket wheels fitting together and "$0.85/hour" on the bottom of the image.]
- Locals may be strong generalists: can be hired for any task that relates to local negotiation or operations and does not require significant computer literacy or summarizing skills (here, local community members conducted networking, ran info sessions, collected data, and trekked to all communities).
[Imagine a Venn diagram with the words "Generalist" and "Specialist" and the intersection label "Magic" crossed and under it written "local contractors."]
- Similarly, NGOs can be provided funding to implement a specific project or recommended specific means to achieve an objective (here, for example, COVID awareness and prevention was a request from the local leadership but the media information part was suggested). NGOs can differ in the cost of implementation by an order of magnitude. For example, 5 hours of data gathering in 8 communities may cost a total of $40 (volunteer stipends plus coordination costs) when conducted by the contracted NGO. Reach Out Cameroon (a larger NGO, $1.8m income in 2019) could charge, for example, $400 for the same task. Small local NGOs may have limited online presence (for example only have a Facebook page but not a website). Accountability can be increased by transparency requirements (e. g. requiring past financial statements) and detailed inquiry regarding spending needs (understanding that at-the-cost quotes may include small surcharges that different persons may benefit from to a limited extent). Double the minimum wage for skilled field staff otherwise working informally can be greatly welcome. Normal local prices should be known (e. g. $2/return trip for local transport, $35/1,000km for distance bus, $1/1GB of internet data, $0.1/A4 B&W page). Or, different NGOs can be invited to provide a quote and operations particulars and the best fit one contracted.
[Imagine a comparison of a person holding two 10,000 CFA franc banknotes and another holding twenty of such banknotes. Labeled as "Contracted NGO" and "Other NGO offer," respectively.]
- Relatedly, local NGOs may be constrained by skills and scale-up initiative in effecting cost-effective impact more so than by funding. For example, the newspaper article could have been ‘sold’ to the paper as a general contribution as opposed to purchased as an ad. Further, this article could have been shared with papers in similarly uninformed localities across Cameroon to increase awareness levels. Analogous measures could have been taken with the radio show (anecdotally, the local station offered a free-of-charge extension (double the time it runs) to the show). Thus, developing liked and beneficial media resources and sharing them with local networks through personal conversations may be particularly cost-effective.
[The image of the information on COVID-19 in the local newspaper with a green letters "Print for free?" over it.]
- Also relatedly, conducting a robust statistical evaluation can be affordable even to small NGOs.
[Image of documents with "Robust evaluation easy?"]
- When statistically evaluating a project, focus on one (or a few) representative measurable outcome (here, mask wearing as a proxy to all preventive measures). Gain other information to optimize the project/clarify fundamental issues in addition (here, we used only one variable from the 64 and we learned what we needed to know (e. g. general beliefs regarding COVID, sources that inform behaviors) from the organizer who works in the area. This approach can be also preferred by local employees (why would they spend a significant amount of time asking locals about what all parties know that the enumerators already know).
[Image of a target with "Measure one outcome."]
- Conduct programs and impact evaluation in a way that discerns what has worked (we do not know what combination of program aspects (radio, newspaper, posters, in-person) worked to what extent. Ideally, we would thus estimate additional cost-effectiveness conditional on other measures and optimize for total cost-effectiveness (for example, we could find that when locals hear a show in a radio, it only takes a poster at the community center by the community leader to change behavior; that when volunteers operate in person, radio and newspaper has no significant additional impact; or that when radio, newspaper, and poster campaign is run, volunteers are received poorly due to the perception of ‘persistent advertisement’ of a ‘foreign’ measure).
[Image of different radio, poster, in-person conversation, and newspaper combinations, with the words "Cost-effective?"]
Image credits
Soldiers in masks, Moki Edwin Kindzeka, VOA, March 07, 2021
CFA Francs exchange, Thierry Gouegnon PW/SM /Reuters, Al Jazeera, 12 Jul 2019
Persons outside, Vatican News, 25 September 2019
Dream team gears, Creativedge Training, 6 September 2014
Specialist generalist, Fizzle Co., Corbett Barr
2×10,000 XAF, Joël Té-Léssia Assoko, The Africa Report, 2 December 2020
10×10,000 XAF, René Nkowa, from douala with love, 12 March 2020
January 28, 2021, update:
The project has been run and follow-up survey data in most communities collected. We should update this post with impact evaluation.
September 21 update:
The Santa Division has been under lockdown for two weeks, since September 7. No cars or motorcycles are permitted to operate. The project will continue when the restrictions are lifted.
September 6 update:
EA Cameroon collected baseline data and is looking to start campaigning this week. If you are interested in working with us on baseline data analysis (Excel), please comment on this post or let brb243 know via the EA Forum.
August 23 update:
The radio show in the seven (added one) locally-spoken languages...
[Team preparing for radio recording image.]
[Radio recording image.]
... has been recorded.
We are waiting for the conclusion of baseline surveys to start broadcasting the show. Further project updates will follow.
August 14 update:
The funds were processed. We will update with baseline data and other project particulars once these are available.
August 7 update:
We are waiting for funds processing at the Cameroonian bank headquarters. We will update when the funds can be collected and the project can start.
July 25 update:
We (at least temporarily) stopped fundraising. Based on the raised amount USD 3,650 (after the GoFundMe 2.9% + $0.3/transaction processing fee, including a USD 640 bank-transfer donation), we updated the tentative budget:
[Budget image (for 1 month): Total funds: $3,650, radio show: $1,280, posters: $520, flyers: $200, volunteer stipend: $480, transportation: $100, miscellaneous: $30, subtotal: $2,610, remaining after 1st month: $1,040.]
After one month, we will estimate the cost-effectiveness of the campaign and compare it to that of the DMI's COVID-19 program. If the cost-effectiveness may be comparable, we will see if we can meet any remaining project needs with the remaining funds (USD 1,040, or 28% of the currently available amount), if we require further funding, or if campaign should be extended to other areas. If DMI's program is more cost-effective, we will inquire funders of the remaining amount about further steps.
Currently, newspaper poster & flyer graphics are finalized, radio show transcript is almost finalized, detailed information about COVID-19 preventive measures for community leaders can be shared in its current form, and M&E baseline and midline questionnaires are drafted.
Feel free to comment on any of this material.
We are waiting for bank transfer processing. Ideally, we would like to start the program at the end of next week.
July 9 update:
The Development Media International's COVID-19 prevention campaign (28:52) uses, marginally, about USD 0.017/person informed. The cost per life saved is between $50 and $1,000 (31:55–32:20). In comparison, EA Cameroon's cost is USD 0.0283/person. However, EACAM adds personal delivery of informational flyers to local community leaders, workshops on making own masks, and newspaper articles. Also, if only some of the activities to inform the Santa community are selected, the cost/person will decrease. Thus, donating to EA Cameroon for the COVID-19 prevention campaign may be the most cost-effective way to provide a quality life that is currently available.
Counterarguments: However, newspaper articles may already exist (as per EACAM, none on prevention), flyers may be too few (if shared in-person while talking with local community leaders, the flyers may be well regarded), and workshops may be better run via radio (it may be difficult to explain what piece of fabric to put where, videocalls are not possible because of very low smartphone/computer use).
So,
deliberate carefully, potentially donate now
Use the GoFundMe link above or message brb243 if you wish to donate via a US or EU bank transfer or an international transfer to Cameroon.
--> Also, please, do let us know why you choose to support any parts of this project or to refrain from doing so. Also, please tell us if we can help even more cost-effectively. We can possibly make it happen.
Summary
EA Cameroon aims to inform 180,000 individuals in the Santa Division of Cameroon about COVID-19 and its prevention measures. Since virtually no prevention information has been shared so far, we aim to reduce new coronavirus cases 35×. For 4 months, we plan to run 3 talk shows in local languages per week, post one infographic article in local newspaper per week, distribute 1,000 flyers to local community leaders, and run 2 workshops on making own masks.
We have radio talk show experience, infographic writing skills, community connections, organizational expertise, and relevant linguistic knowledge. The only thing that is missing is funding.
We require USD 5,090 (USD 0.0283/person) to manage all of these prevention measures. This includes all costs and overhead.
Please donate now via GoFundMe, or message brb243 for US and EU banking details. Let us know regarding any possible support (for particular activities or otherwise) or feedback in the comments below, at ea.cam@yahoo.com or call Alex at +237652263908. We will appreciate any prompt responses since in Cameroon, coronavirus cases are increasing at the second highest rate in Africa (after South Africa).
[Team image, in masks.]
Project details
EA Cameroon plans to inform 180,000 individuals in the Santa Division of Cameroon about COVID-19 and its prevention measures. We aim to reduce new coronavirus cases 35× (https://www.washingtonpost.com/nation/2020/05/15/social-distancing-study-coronavirus-spread/).
We (core EA Cameroon and trusted community volunteers) plan to manage these 4 activities for 4 months:
· Run 3 30-min radio talk shows per week in local dialects, Pidgin English, and English.
· Write weekly COVID-19 situation update and prevention reminders in local newspapers.
· In-person distribute 1,000 flyers to trusted village leaders while raising their awareness of COVID-19 and talking to them about effective prevention measures that they can share with their communities. We will trek to several communities because of poor conditions or the absence of roads.
· Run 2 workshops on making own masks while maximizing social distancing.
At the time of submission of this proposal, none of these four measures took place in the Santa Division. Social distancing has not increased: people are crowded in the markets, at local njangi (associations), shops, funerals, etc. Only one in five wears a mask. Further, citizens hesitate to trust government statistics on the disease.
Concurrently, COVID-19 cases in Cameroon are increasing at the second highest rate in Africa (after South Africa), with regards to daily surge. On July 6, 2020, Cameroon has confirmed 13,711 cases. The death toll from the virus rose to 328 after 22 more patients died in the last 24 hours. 11,114 patients are currently recovering. The Santa Division has confirmed 720 cases, 350 recoveries, and 28 deaths.
We propose to leverage existing human and information infrastructure resources to reverse the trends in the spread of COVID-19 in the Santa Division of Cameroon (villages Akum, Meforbe, Santa, Pinyin, Njong, Bamock, and Mbei).
Our Track Record
EA Cameroon comprises experts from various fields who are caring, loving, and aimed at doing good to humanity and the environment. Since 2017, we have been assisting the poorest members of the Santa Division’s rural communities to meet their various needs. With little available resources and extensive local knowledge, we maximize our operational cost-effectiveness, responding to the greatest and most neglected needs.
Relevantly to the proposed project, last month, we distributed 180 masks to people in 4 communities. Recipients are wearing them. Unfortunately, most persons had to be turned down because of the mask shortage. Thus, running workshops on making own masks from available materials may be more suitable in Santa.
In the past, we run radio talk shows on climate change, children’s rights, and gender equality. Our members speak many of the local dialects and can organize translation into languages that we do not speak. We will be delighted to share WHO Africa’s COVID-19 prevention recommendations with our friends who shall be happy to hear from us again.
Additionally, we can make COVID-19 prevention infographics for local newspapers, publishing them as ads. We can adjust these as flyers that we plan to bring to and talk about with village leaders that we meet through our connections.
Traditionally, we have relied on local sources and volunteer commitments to run our activities, building on existing community assets to improve the community life. However, the COVID-19 Awareness and Prevention project requires external support. Since other actors are not likely to step in at this point of the local coronavirus spread, or at all in remote villages, we offer a great opportunity for making cost-effective impact in COVID-19 prevention.
Other Team Members
[July 21, 2020 edit] In addition, brb243, an EA volunteer with 8 years of international development work and study experience, is supporting this project online.
[July 26, 2020 edit] Pim, an instructional designer, is working on the graphic design.
[August 7, 2020 edit] Malvya Chintakindi and Sayak Khatua of 3ie are consulting on impact evaluation.
Proposed budget
[Proposed budget image, $5,090 total. Items: radio show $1,920, newspaper $720, flyers $200, workshop $200, volunteer stipend $1,920, transportation $100, miscellaneous $30.]
Contact details
E-mail: ea.cam@yahoo.com
Phone: +237652263908 (Alex Gwanvalla, EA Cameroon organizer)
Please contact us anytime (or comment below) with any collaboration offers or/and feedback on our activities. We welcome any support, for particular measures or otherwise.
This looks like a great initiative!
I noticed that based on the link in your EA Forum profile, you're located in the Czech Republic--would you mind talking a bit about your relationship with EA Cameroon?
Sure! I am currently connecting with EAs in sub-Saharan Africa with the intention of building the EA community there. During these conversations, I identified a project that the EA community may be interested in and offered to edit the writing of EA Cameroon.
Meta-level: It might help to add a section on the top explaining the above so the relationship is clear.
Added the [July 21, 2020 edit] to the Our Track Record section that talks about the team.
It's nice to see the photo - is that the team, and are there more details about the people doing the project somewhere?
What will be the monitoring and evaluation of outcomes, and how will spending be accounted and tracked.
Hello Ray,
That is a part of the team. Community leaders (not pictured) will be also engaged in recording the show in local languages and answering questions regarding details of any of the preventive measures in their local communities.
The idea is to collect baseline data on following the preventive measures (and case incidence, if possible) in a town within the radio and newspaper reach and in a comparable town outside of the reach of the two. After one month, the results will be evaluated and further steps taken accordingly.
The spending will be accounted and tracked by EA Cameroon. It may be a great idea to post updates on spending.
Since you requested feedback, here are some quick thoughts:
While I very much hope Cameroon is able to bring COVID under control, it seems like this could be difficult based on what we've seen in other countries. So the part of your plan that I'm most optimistic about is the mask making, because I think that could save lives even if COVID is not brought under control. Somewhere I read (can't remember where unfortunately) that if you wear a mask, then you'll end up inhaling a smaller number of viral particles if you get exposed to an infected person, and inhaling a smaller number of viral particles tends to give you a milder case, which means you're more likely to acquire immunity without putting your life at risk.
So I'd encourage you think about questions like: After we practice explaining the mask-making process in our workshops, can we find a way to explain mask-making via radio / flyers / newspaper articles? Or can we tell everyone at our mask-making workshops that they should run their own mask-making workshops for their family and friends and so on, so the mask-making knowledge spreads through the population that way?
Additionally, from what I've read some homemade masks are much more effective than others. Some snippets from my notes on mask effectiveness:
https://www.nationalgeographic.com/science/2020/07/how-to-make-coronavirus-masks-that-everyone-will-want-to-wear-cvd/
https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/coronavirus-face-masks-what-you-need-to-know
https://www.sleepphones.com/Comfortable-Coronavirus-Face-Mask-Beard-Glasses-Fogging
https://www.nytimes.com/article/coronavirus-homemade-mask-material-DIY-face-mask-ppe.html
https://www.medrxiv.org/content/10.1101/2020.04.17.20069567v2.full.pdf
So it's probably worth doing some research to figure out the best mask design from the perspective of effectiveness, ease of explaining how to create, and likelihood that people in the Santa Division will be able to acquire the necessary materials, if you haven't already done this.
Hi John,
This is so cool! Actually EA Cameroon has done this research and they recommended using socks. However, all the resources will specify that any fabric works, as long as it covers mouth and nose.
And yes, I should write an update. The mask-making will be explained via radio and also taught to community leaders who will then be able to run the workshops. It is actually a great idea to schedule these workshops. Everyone will be encouraged to share the general information regarding preventive measures.
Hm, socks are knitted not woven, right?
Yes. In terms of percentage, how less effective are 4 layers of woven fabric in preventing the spread of coronavirus than 4 layers of knitted fabric? Than 2 layers of woven fabric? The idea is to have at least 4 layers of the sock (after folding) or at least 2 layers of other fabric. In preventing breathing in the virus?
I have no idea, I already shared my notes above! :) Perhaps the team could reach out to e.g. the author of the Johns Hopkins article?
BTW, I did find this article which argues for knitted masks:
https://stringking.com/face-masks/knit-vs-woven-fabric/
However, I'm more inclined to trust Johns Hopkins. But maybe the author of the Johns Hopkins article would have interesting opinions on the above link.
Edit: Here's more info
https://med.stanford.edu/news/all-news/2020/06/stanford-scientists-contribute-to-who-mask-guidelines.html
OK, thank you. Added that better fitting masks made of denser material work better.