This is a Draft Amnesty Week draft.It may not be polished, up to my usual standards, fully thought through, or fully fact-checked. |
Commenting and feedback guidelines:
|
Problems with my draft:The biggest problem is that I haven't got the sources done and polished. There are more claims than there are sources. That doesn't mean that they are false, just that they are weak. I haven't put the time into deeply reading each source and making sure each claim meets a rigorous standard. While I believe what I am saying, meeting a high scientific bar is a long process that I do not forsee myself getting around to doing. As a result, I am publishing this post in draft form.
Since I started writing and shelved the project, new sources now exist with new numbers i.e. - https://pubmed.ncbi.nlm.nih.gov/27568340/
I would love other people to look into this I would love other people to champion the idea and take it from me. I would love someone to spearhead the future of this work.
My google doc with many more comments/scrutinizing can be found here: https://docs.google.com/document/d/1fxjvnWlGeSAZxrUiB30eogF0urry5_ZPjGzZpui0NsQ/edit?tab=t.0
|
Craniofacial health as a neglected global health intervention
The prevalence of orthodontic treatment, largely for cosmetic reasons, during a lifetime may be reaching 20% in the United States with the “need” much higher (Brunelle et al. 1996, Christopherson et al. 2009). - The Jaw Epidemic: Recognition, Origins, Cures, and Prevention from the journal Bioscience by Oxford University Press 1
Brief summary
Problem:
Humanity faces a shrinking jaw epidemic with disastrous health consequences. At least 20% of the population has jaw formation problems, mainly caused by changing dietary patterns as societies industrialise and the lack of hard foods combined with growing allergies from living indoors. This is perceived as a cosmetic issue to be fixed by braces but this is actually a medical issue with serious health consequences.
The health consequences of underdeveloped jaws may include sleep apnea, asthma, ADHD, allergies and sensitivities, breathing problems, anxiety and more. These health consequences are linked to major financial impacts on the global economy.
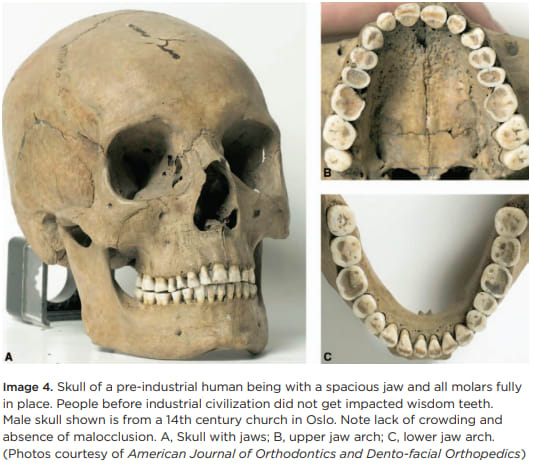
The orthodontic industry is incentivised to treat symptoms rather than root causes. It’s common practice in developed countries for wisdom teeth to be removed. The standard story that wisdom teeth would have taken the place of a fallen out tooth, does not agree with the historic skull records (Weston A price in peru: “In an examination of one thousand two hundred and seventy-six skulls in succession I did not find one with the typical deformities of our moderns.4”).
Scale of problem: 20-50% of adults in developed countries, developing countries also form similar problems because they replicate the western diet.
Why we haven’t tackled the problem so far or what we’re doing wrong:
Lack of awareness of the problem on an individual level, Orthodontic industry business model on a systemic level, laziness on a societal level, incorrect model of craniofacial development and treatment on a global scale.
A Better Solution: One proposed solution is Mewing, a set of free guidelines for improving jaw muscle and posture. This improves sleep, breathing, anxiety and beautifies the face.
Significant population segments include babies (when breastfeeding and growing teeth), children (when habit forming) and teenagers (during bone growth phases). Individuals over the age of 25 can expect some improvement although slower.
Relevance to EA
My estimate of the ITN score (higher is more important to be addressing because it’s more solvable and promising)
Scale score:8-12/16
Neglectedness: 12/12
Solvability: 6-8/8 (this is unusually high because the problem is so neglected, a tiny amount of more work/support can make a huge difference)
(see more in: ^^^ Scale, Solvability and Neglectedness)
Scale, solvability, neglectedness
This impact area is at a high scale affecting as high as 1 in 5 people in America. The jaw epidemic seems highly solvable with Mewing. There’s nearly nobody working on this and so this intervention could yield high results.
This could be a new EA cause area
We propose a new EA public health initiative to solve this issue. We’re looking for advocates to help with dissemination of information to paediatricians, general medical professionals (particularly sleep doctors), orthodontists, and the general public. If you want to contribute, please ^^^get in touch at the end of the document.
Our Current Jaw Context
- This is a modern issue - not genetics. Can see the changes within 1 - 2 generations.
- Our diet’s role: Our food is too soft now
- Current methods to solve jaw issues
%Modern Jaws are shrinking. Look around.
%Statistics. Rates of braces,
%Wisdom teeth are commonly removed.
%Photos of ancestral vs current populations
Historic Background
- Historic rates of jaw issues (Archaeology and Anthropology)
When we look at either tribal cultures or the skeletons of older cultures, we don’t find underdeveloped jaws at all. When we look at the current population we find massive numbers of jaw issues..
Anecdotally today, shrinkage has been observed in one generation (Waugh 1937) or within a single individual.
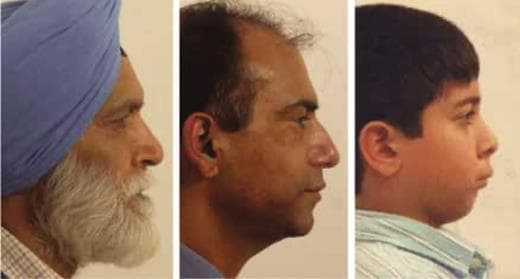
Indian Grandfather born in village who had come to England as a young man with his children. Son in center. Grandchild (right) was born in industrialized society. You can see a progressive reduction in the forward dentofacial growth in the three generations. Photographs: John Mew.
For rates of jaw issues in the population (see ^^^Statistics of affected population)
From The Jaw Epidemic oxford bioscience paper (Authors: Sandra Kahn, Paul Ehrlich, Marcus Feldman, Robert Sapolsky, Simon Wong):
Despite claims that the cause of this jaw epidemic is somehow genetic, the speed with which human jaws have changed, especially in the last few centuries, is much too fast to be evolutionary. Correlation in time and space strongly suggests the symptoms are phenotypic responses to a vast natural experiment—rapid and dramatic modifications of human physical and cultural environments. 1
From The Jaw Epidemic oxford bioscience paper (Authors: Sandra Kahn, Paul Ehrlich, Marcus Feldman, Robert Sapolsky, Simon Wong):
The mechanism of change, research and clinical trials suggest, lies in orofacial posture, the way people now hold their jaws when not voluntarily moving them in speaking or eating and especially when sleeping. The critical resting oral posture has been disrupted in societies no longer hunting and gathering. Virtually all aspects of how modern people function and rest are radically different from those of our ancestors1
Bones grow (and change shape) under light but persistent pressures. Those created by oral posture—the positions of the jaws and tongue in relation to each other when a child is not eating or speaking—constitute signals that, among other signals, guide the growth of the jaws.
What Mew (2004) postulated and more recently Engelke and his colleagues (Engelke et al. 2011, Knösel et al. 2016) have demonstrated as “correct” oral posture is holding the teeth lightly together, with the tongue positioned against the palate; clinical studies show that this posture results in an adequately roomy jaw (Wong 2018).
Humanity cooks and processes food more than ever. Leaving little work to our jaws. Jaw bones (and all bones) grow in response to:
(1) Passive resting forces
- The tongue
- The upper and lower teeth in light contact grow
(2) Active chewing forces exerted on them.
- The force applied when chewing
- The tongue movements when eating and drinking
Together these guide healthy craniofacial development. With jaws growing forward and laterally.
%Image of forward and healthy face vs retruded face?
Modern disruptions to these natural forces have altered our jaw development. Human jaws have been shrinking since hunter gatherer days and this has accelerated in recent times for the following reasons:
- Increasing processed foods and soft foods which are swallowed quickly without adequate chewing and provide little work for the jaws
- Reduction in breastfeeding - being replaced by bottle feeding which sets a child up for improper feeding habits and weak facial muscles and jaws (a bottle delivers milk without the natural latch and sucking behaviour)
- Allergies from modern conditions** which leads to blocked noses and sinuses. In response we breathe through our mouths as a compensation mechanism to survive. Which disrupts the resting oral posture and jaw growth.
**It’s open to scientific debate as to which modern conditions are to blame for allergies but theories include some or all of; dust, pollution, urbanisation, pets, vitamin deficiencies, antibiotic use, plastics and more.
From The Jaw Epidemic oxford bioscience paper (Authors: Sandra Kahn, Paul Ehrlich, Marcus Feldman, Robert Sapolsky, Simon Wong):

Allergy can block a young person's nostrils as thoroughly as plastic plugs can block those of a rhesus monkey. Look at the consequences in the present figure for an attractive youth (left) getting a gerbil for a pet. He was allergic to the gerbil, and the resulting nasal congestion and mouth breathing redirected the growth of his jaw with sad results (center and right). Photographs: John Mew.
…
Nonhuman animals that had their oral posture disrupted by nose blockage or a dietary manipulation (Harvold 1968, Lieberman DE et al. 2004) showed changes in their jaws analogous to what is happening to children in industrialized societies today (Grippaudo et al. 2016, Kahn and Ehrlich 2018).
Consequences
These disruptions to swallowing patterns, resting tongue posture and forces on the jaws lead to weak jaw muscles and underdeveloped jaw bones, tongue muscles and Malocclusion (abnormal alignment) of teeth. So called Craniofacial dystrophy.
Without the tongue providing forward force and lateral (sideways) forces the jaw bones don’t develop properly. The upper jaw - the maxilla becomes… The palate raises. The lower jaw is held back by the upper jaw position….
Teeth then get crowded - as the jaw bones they sit in are too small. Without adequate forward growth the wisdom teeth don’t emerge properly. Our faces rotate downward and we have a “longer” face.
The resting tongue posture acts as a scaffold for shaping the layout of the teeth.
https://tooth-for-a-tooth.com/wp-content/uploads/2020/12/7D01B097-0B68-427E-AA76-8BDD37F3FC82.jpeg
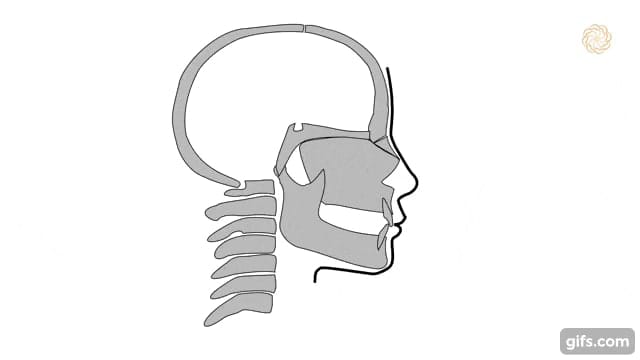
When the tongue moves away from the roof of the mouth, the tongue falls back into our mouth and throat. For those lacking forward jaw growth this blocks their airways. To compensate for the blocked airway the neck leans forwards and the head tilts upwards to open the airways during the day. This creates body posture issues (neck, head, shoulder tension) but at least keeps us alive.
This posture adaptation doesn’t work to open the airways during sleep when we are lying down and we mouth breathe and snore, developing sleep disordered breathing and sleep apnea.
Our brain experiences changes in blood flow and oxygen levels. Undergoing periodic starvation of oxygen during sleep (hypoxia) which has profound consequences on brain repair and functioning.
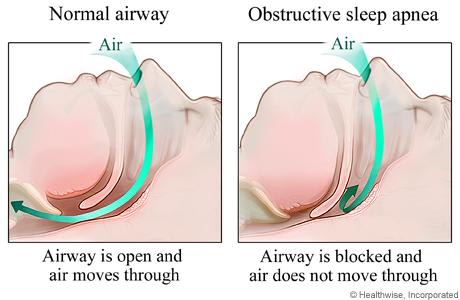
During sleep the airway can collapse causing a number of flow on effects.
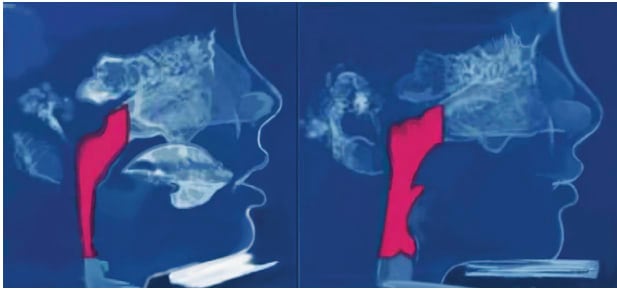
On the left is a narrow airway and on the right is an improved airway after treatment.
%We could annotate this diagram + include a caption about optimal vs unhealthy.. Pre and post treatment..
The consequences of this are:
- We wake up tired, with an overactive stress response, poor mental/physical health, symptoms of stress, gut issues, skin issues, heart issues + much more. Lost lifespan + productivity due to health problems.
- We present with the symptoms of ADHD - poor executive functioning, impulse control, trouble regulating emotions, low energy and easily fatigued during the day
- Heart failure is tied to OSA
- Mouth breathing bypasses the filtering effects of the nose - increasing our risk of infections. While also setting us into fight or flight mode (as if we were running).
- "When you can't breathe through your nose you are forced to breathe through your mouth. This inhibits parasympathetic breathing and, in turn, activates your “fight or flight”, keeping you from getting restful sleep. The root cause of an underdeveloped upper airway is often an underdeveloped jaw." Source: https://ecologicdentistry.com/the-importance-of-parasympathetic-breathing
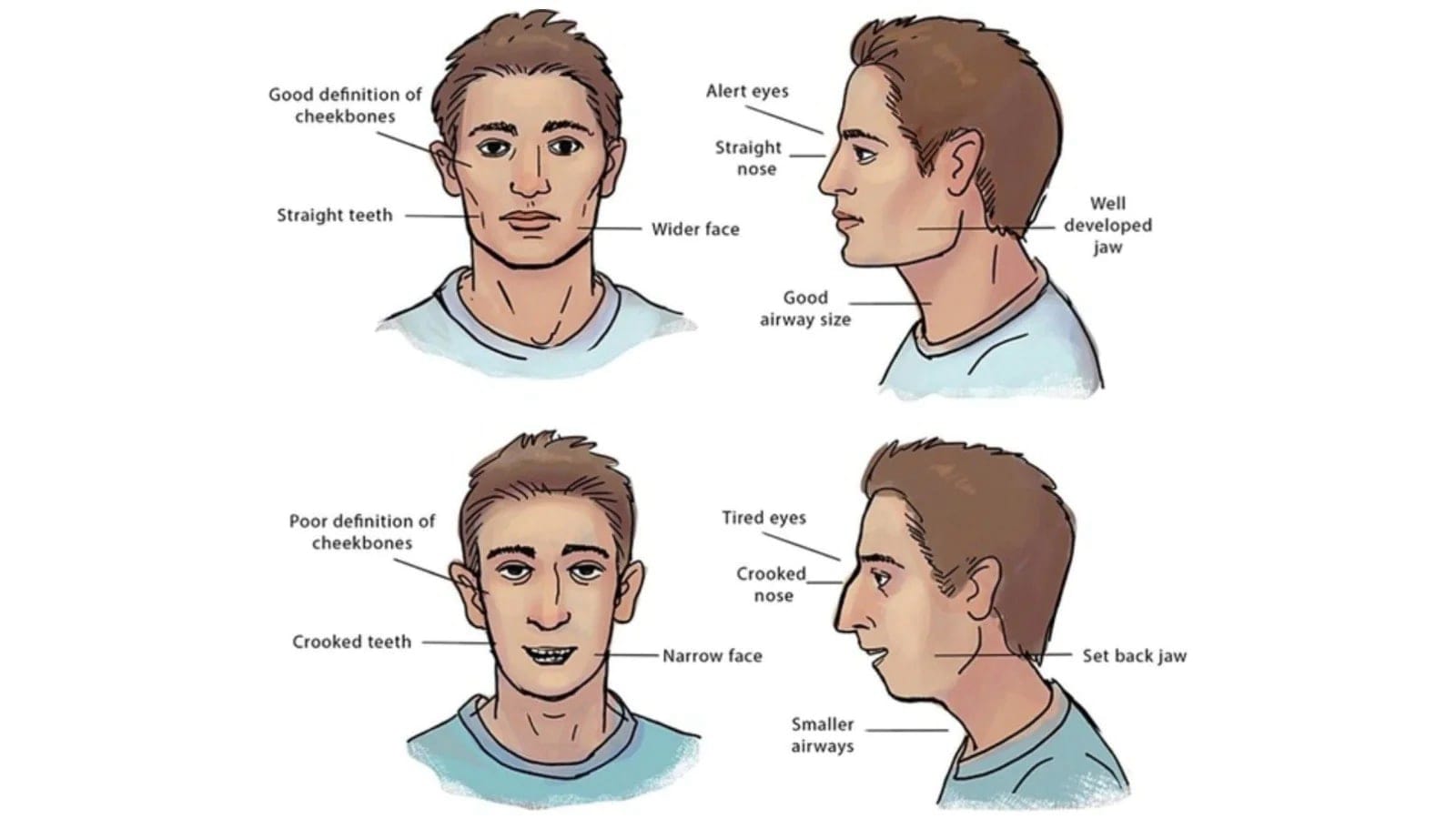
- As a result of this underdevelopment, facial features look less attractive. We are wired to find healthy development more attractive.
These consequences can grow worse over time.
Relevant health conditions
See the book Jaws for more information.
- ADHD
- Sleep related breathing disorders - and it’s impacts on mortality
- OSA
- UARS
- Allergies
- Depression/anxiety from inconsistent airflow during sleep
- Crooked teeth
- Incorrect wisdom teeth formation
Statistics and quantification
In a 1996 paper in the Journal of Dental Research “almost 20% of adults ages 18-50, as well as 18% of children, have had orthodontic treatment.”2
- The worldwide prevalence of malocclusion was 56% (95% CI: 11-99), without differences in gender. The highest prevalence was in Africa (81%) and Europe (72%), followed by America (53%) and Asia (48%). Source
- Statistics estimating population with conditions:
- Sleep problems
- The prevalence of obstructive sleep apnea appears to be perhaps 2%–7% or more in children (Lumeng and Chervin 2008), about 5%–20% in adults in general (Finkel et al. 2009), and over 80% in some elderly populations (Senaratna et al. 2017) Source
- Sleep Disordered Breathing/Obstructive Sleep Apnoea
- almost 1 billion people affected, and with prevalence exceeding 50% in some countries. Source
- You are 3.8 times more likely to die from all cause mortality if you have sleep disordered breathing (SDB) than if you do not. Source (Sleep Disordered Breathing and Mortality: Eighteen-Year Follow-up of the Wisconsin Sleep Cohort - PMC)
- Adhd -
- The global prevalence of ADHD ranges from 1.2 to 7.3% Source
- The prevalence of sleep disorders in children with ADHD ranges from 35 to 70% Source
- [T]he prevalence of persistent adult ADHD was 2.58% and that of symptomatic adult ADHD was 6.76%, translating to 139.84 million and 366.33 million affected adults in 2020 globally. source
- Anxiety
- [T]he total prevalence was 4802·4 cases (4108·2 to 5588·6) per 100 000 population. Altogether, major depressive disorder caused 49·4 million (33·6 to 68·7) DALYs and anxiety disorders caused 44·5 million (30·2 to 62·5) DALYs globally in 2020. Source
- An estimated 4.05% of the global population has an anxiety disorder. Source
- Speech defects
- Nearly 1 in 12 (7.7 percent) U.S. children ages 3-17 has had a disorder related to voice, speech, language, or swallowing in the past 12 months Source
- Allergies
- Sleep problems
- Statistics estimating number of surgeries and or other invasive treatment methods
- It is estimated that nearly 5% of the UK or US population present with dentofacial deformities (wikipedia sources the textbook “Orthognathic Surgery. Principles and Practice” Jeffrey C. Posnick - source unconfirmed)
- In Sweden: The population-prevalence-rate of orthognathic procedures over the 5-year period was 6.3 (SD 0.4) per 100,000 persons Source
- Economic cost of allergies
- Allergies
- In per capita terms, this amounts to a financial cost of around $1,912 per person with allergies per annum. Including the value of lost wellbeing, the cost is $7,200 per person per annum. Source
- Allergies
- [other relevant statistics]
- General Dental costs
- Improvement in oral health alone can offer the world substantial economic benefit as researchers have estimated that the yearly global economic impact of dental diseases amount to $442 billion. Source
- aggregate country‐level expenditures in 2015 were the highest for the United States (US$109.4bn), Germany (US$29.5bn) and Japan (US$25.6bn) Source
- General Dental costs
A model of Impact
This is an approximate model:
(affected population, or population affected by related conditions) * (QALY improvement) / (possibility that the treatment doesn’t work). = positive impact
Affected population of Jaw issues = 1 in 5 or higher in the US, (up to 90% of kids in saudi arabia)
Some conditions:
- Sleep apnea: 5-10% of people worldwide.
- Adhd 16% of children in america https://www.cdc.gov/ncbddd/adhd/data.html
- Anxiety 31% of adults
Some number of QALY improvements.
If I take the minimum numbers and suggest I could solve a fraction of global sleep apnea, for example if only 1 in 10 people actually try mewing and improve their condition, the benefit to humanity could be massive.
The Current Orthodontic Approach is Inadequate
- Rather than growing faces forwards and wider - “retractive” dentistry has been focused on extracting teeth to create space and then moving other teeth back into this space. Thus moving faces backwards. Which creates problems later on. Braces don’t solve the underlying problem of underdeveloped jaws - they move the teeth, not fix the jaw bone. They can cause root resorption decades down the line from exerting constant unnatural forces on dental roots. Teeth are just the symptoms of small, underdeveloped jaws. When we instead fix the jaws - teeth which sit in the jaws will have plenty of space and fall into the right place.
- The orthodontic industry is cosmetically focused on treating symptoms rather than preventing the condition by examining root causes. The economic incentives lead to extracting teeth (), versus prevention (of a previously unclear cause) by shifting behaviour patterns, lifestyle and environment.
- Dentists are not cross trained with ENT (ear, nose and throat) knowledge of the structure of the skull and address the problem only from the perspective of the teeth and mouth.
- “To date, there are almost no treatment approaches that aim for the prevention of jaw development problems. There are no definitive evidence-based interceptive approaches.” Source
- The orthodontic industry has been trained in cosmetic solutions. We need to rewrite the textbooks in orthodontics, retrain orthodontists and change the culture of orthodontic practices so that we can save people money and help empower patients to improve their own craniofacial health.
Raise the alarm
- Not enough is being done. The prevalence of malocclusion is 90% in Saudi Arabia + Nigeria according to some studies.
- The issue is expensive to treat once developed ($1000’s for braces, palate expanders), (($10,000’s for surgery). Versus cheap to free with Mewing when caught earlier.
- This is a public health issue that needs a public health intervention. From education of the public to educating dentists + shifting dental/food policy.
A Better Solution - From Extraction to Expansion
Given we understand the mechanisms at work - solutions naturally arise.
There is a growing movement called “Mewing” named after the pioneering father-son orthodontist duo - John and Mike Mew. It signifies a shift from Orthodontics and Extractive Dentistry to what is now termed “Orthotropics” and Craniofacial Expansion. It’s centred around the premise that:
- Lifestyle and our environment are the problem. Not our genetics.
- Avoid extractions where possible
- Create space (for the teeth) by expanding the maxilla and cranial bones
- Start earlier to maximise the likelihood of success. Young faces are very malleable especially during puberty. The older we get the slower our bones change.
Mewing consists of the following behavioural interventions:
- Chewing hard foods
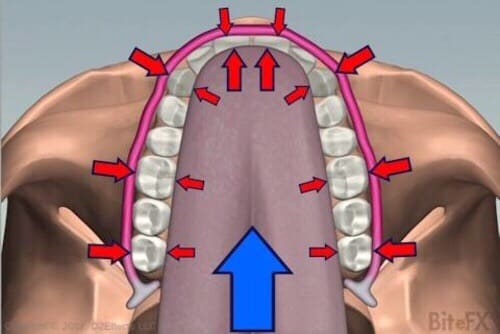
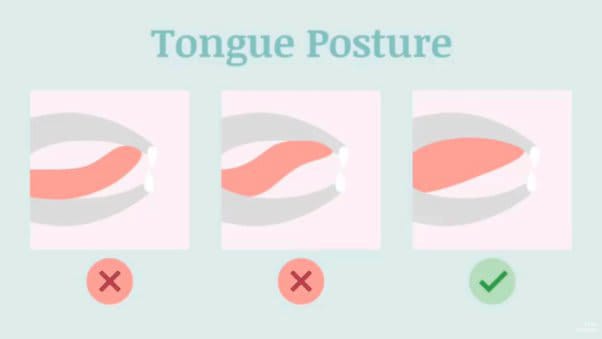
- Resting tongue posture on the roof of the mouth from front to back (see diagram below)
- Lips lightly touching, teeth lightly touching
- Mouth closed during the day to enable nose breathing
- Nose breathing during wake and sleep (using mouth tape at night if needed)
- Establishing a proper swallowing pattern - rather than sucking
- Standing up straight with head up and shoulders back
Correct resting oral posture |
Success also requires:
- Detecting and correcting for any allergies that lead to blocked noses and mouth breathing from dust to pets to food allergies
- Increasing nutrient intake (Vitamin K2 + Calcium) + ensuring adequate sunlight (Vitamin D)
- Potential sleep studies to ascertain sleep disorders
Challenges and Failure Modes:
The earlier this is detected and treated the better the potential outcomes. Young faces are very malleable especially during puberty. Cranial bones start to fuse over time and the older we get the slower our bones change.
Many adults see profound changes over time as evidenced by viral images and videos but when struggling with debilitating sleep apnea - it can be hard to wait the years required for improvement.
When jaws are underdeveloped and teeth are crowded - the mouth is too small for our tongues and it can be difficult to “Mew” and place the tongue in the right posture. Dr.Felix Liao has termed this the “Six-Foot Tiger in a Three-Foot Cage”.
That’s where Dental appliances like Palate Expanders are used alongside mewing to apply persistent forces for much of the day to grow our upper/lower jaws. These costs $1000’s.
Often a fixed device such as the MSE Expander is attached to the upper jaw via surgery and a screw is turned to increase the width of the device and thus spur rapid palatal/jaw expansion.
There are also removable appliances like the Homeoblock or the Vivos DNA appliance that can be worn during sleep or 8 - 16 hours a day. They exert a spring like light forces on the teeth and the proposed mechanism is this signals jaw growth.
One of the authors of this document has personally experienced the Homeoblock appliance and benefitted tremendously but has heard anecdotal reports from others for whom the appliance didn’t work as well or tipped their teeth. (^^^ See Personal)
Further research is needed on the effectiveness of these devices.
These often need to be followed by braces to correct teeth once bone expansion is completed. Which also cost $1000’s.
In some cases jaw surgery may be needed (Maxillomandibular advancement surgery (MMA)) to correct the jaws. This can cost $30,000 - $60,000+.
To reduce the cost of this global intervention we’ve decided to focus on craniofacial education as its cost is between cheap and free because it’s a public health information initiative that can be done at scale and not a surgical or individual intervention.
“The worldwide high prevalence of malocclusion and its early onset during childhood should induce policymakers as well as paediatric physicians and dentists to devise policies and adopt clinical strategies for preventing malocclusion since younger children's ages.”
From: Worldwide prevalence of malocclusion in the different stages of dentition: A systematic review and meta-analysis https://pubmed.ncbi.nlm.nih.gov/32567942/
Mewing evidence (to organise from the reference section)
- Case studies
- Papers
- Before and after photos

Current evidence suggests that alteration of oral postural influences on skeletal growth is the main cause of malocclusion. It results from changes in the persistent but gentle forces that appear to influence phenotypic skeletal development—soft tissue positioning molding bone shape and size (Sankey et al. 2000, Mew 2004, 2015a, Buschang et al. 2013, Buschang and Jacob 2014, Pisani et al. 2016). Source
Bones grow (and change shape) under light but persistent pressures. Those created by oral posture—the positions of the jaws and tongue in relation to each other when a child is not eating or speaking—constitute signals that, among other signals, guide the growth of the jaws. What Mew (2004) postulated and more recently Engelke and his colleagues (Engelke et al. 2011, Knösel et al. 2016) have demonstrated as “correct” oral posture is holding the teeth lightly together, with the tongue positioned against the palate; clinical studies show that this posture results in an adequately roomy jaw (Wong 2018). Source
Critiques of mewing
Common critiques of mewing and some simple counter arguments.
It’s all fake, and the before and after photos are surgical intervention.
Mewers don’t have anything to gain from faking their before and after photos. The progress of mewing influencers matches the case studies by John Mew. Mewing influencers may gather an audience but there is no incentive for influencers to convince people to mew. Mewing is cheap and free to do, there’s nothing to sell other than harder foods.
Adults can’t change their jaws.
Adults will only be able to slowly change their jaws but it is possible.
It’s going to be painful, for example TMJ.
Some people who try mewing techniques seem to cause themselves TMJ pain. More research is needed and better education is needed to clarify the correct procedures for improving craniofacial health
Mewing creates other jaw issues
Incorrect mewing can create other jaw issues and muscular imbalances. Better and clear education is needed. Some people will still need surgery to correct their jaws but it’s amazing what can be done without surgery.
Mewing causes an obsession with attraction and facial features
Mewing has been largely taken up by proponents who are concerned with their looks. As a side feature those people also will be experiencing better breathing and better sleep. The focus on looks is more of a side effect and it doesn’t seem like a big deal if people are seeing a primary benefit in attraction.
There are major implications for the mental health industry if mewing works.
Many mental health conditions are linked to breathing difficulties. If those breathing difficulties could be improved, so could a myriad of mental health issues. If people can’t breathe well, they can’t enjoy life either. A craniofacial health focus could positively impact the mental health industry as well.
Orthodontics currently work fine, don’t change them.
Current orthodontic practices are expensive and painful. Some don’t even resolve the medical problems because they are cosmetic focused. Orthodontics can only be afforded by those who are of higher socioeconomic society. Ideally mewing will make it possible to cheaply spread the health improvements across society. We really need better education towards dentists and orthodontists as well.
There isn’t enough evidence yet
See ^^^ Levels along the journey of scientific acceptance. We shouldn’t expect to see so much evidence yet because we are at the early adopter stage of acceptance. We are hopefully going to see more evidence soon.
Lack of Scientific Research and Peer-reviewed Studies
Much of the support for mewing comes from anecdotes and online communities rather than scientific research and peer-reviewed studies.
Counterargument:
While it is true that mewing's benefits are largely based on anecdotal evidence, this doesn't mean that the technique is ineffective. The method is relatively new, and further scientific research is required. The growing number of personal success stories should encourage more in-depth research.
Mewing is Just Good Posture
Some critics argue that mewing is just a new name for maintaining good tongue and jaw posture, which has always been recommended for overall oral health.
Counterargument:
Even if mewing is just about maintaining good posture, the fact that it has brought attention to the importance of tongue positioning and its potential impact on craniofacial development is invaluable. Naming the technique has simply made it more accessible and understandable to the general public.
Mewing is not universally applicable
Mewing may not be effective or suitable for everyone, especially those with certain oral or medical conditions.
Counterargument
Like all medical or health advice, one size doesn't fit all. It's essential for individuals to seek guidance from a professional before making changes to their oral posture or routine, especially if they have existing conditions.
The Role of Genetics
Skeptics argue that genetics plays a larger role in facial development than tongue posture, making mewing's potential benefits negligible.
Counterargument
While genetics undoubtedly play a role in craniofacial development, we can look back a short span of time to our living older generation to see healthier jaw development. If this were a genetic phenomenon, we would see similar jaw problems among older people and we do not.
Misinformation and Exaggeration
There are claims in the mewing community that are not always backed by evidence, leading to misconceptions and potentially false hopes.
Counterargument
Misinformation and confusing information exist in the mewing community. Especially as it’s a group of self-experimenting cutting edge innovators. For public education it is essential to differentiate between what is well-established and what is speculative. As more research is conducted, clearer guidelines and benefits can be established.
Mewing may be Overshadowing Other Solutions
By focusing too much on mewing, people might overlook or undervalue other established treatments or interventions that could be beneficial for them.
Counterargument
Mewing is not being presented as a replacement for other treatments but rather an additional tool or preventive measure. Emphasizing the importance of an approach that combines various strategies is key.
Difficult to Maintain Consistently
Proper mewing requires consistent practice over time, which can be difficult for many to maintain, leading to inconsistent results.
Counterargument
Particularly among teenagers who are experiencing ADHD-like symptoms due to their breathing patterns, they are likely to struggle to maintain a mewing habit. While it is challenging initially to grow a habit, with practice and time, it can become second nature. Those who are committed often report noticing positive changes over time.
What evidence could prove mewing wrong
There are existing case studies with xrays which show evidence of jaw growth. There is a small possibility that all existing X-rays are fake. This seems unlikely.
There are many people on google images under the tag "mewing before and after". There's a possibility that these are also fake, although there's upward of 100 photos
Levels along the journey of scientific acceptance
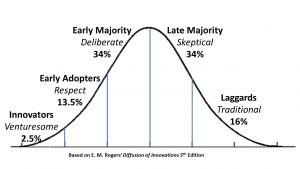
Innovation Adoption Curve - CWBSA
One critique of mewing is that there is not enough evidence. Our simple retort to that is that mewing is at the early adopters phase of idea propagation and there hasn’t been large scale randomised studies conducted yet. Weston Price did his ethnographic research in the 1920s and drew strong conclusions about the impact of diet on health. There's a huge opportunity for more studies to be done on mewing to level it up on the Hierarchy of evidence but more work is needed.
Relevance to EA
Scale, Solvability and Neglectedness
Scale
- Scale 20% of people in developed countries, up to 60% of people accessing dental care
- 50% of people getting braces
- (add more)
Solvability
Are there cost-effective interventions for making progress on this problem with rigorous evidence behind them? (ideally high up the hierarchy of evidence - 1 being the highest evidence and 7 being the lowest).
- Currently we are (arguably) at level 5 of the hierarchy of evidence about mewing. However the evidence is so strong that it’s possible to see the existing studies and skip to level 1.
- We have ongoing case studies about mewing success.
- You only need to type “mewing before and after” into google images to see freely available evidence of jaw changes. They could all be lying but that gets pretty unlikely as the anecdotal case numbers grow.
- We have cohorts of societies who are currently actively growing up with better and worse jaw conditions. We only need to document that evidence more clearly.
Are there promising but unproven interventions that can be cheaply tested?
- Yes. Definitely. This document outlines cheap and promising interventions that could do with more evidence.
Are there theoretical arguments that progress should be possible, such as a good track record in a related area? (e.g. we can’t prove that medical research will be effective ahead of time, but the area has a strong track record, and rough estimates suggest it’s very effective).
- Yes. Animal studies agree with what we see in humans.
Are there interventions that could make a huge contribution to solving the problem, even if unlikely to work?
- Yes absolutely.
Treats some symptoms:
| Intervention | Price |
| braces | $5-6,000 average per person |
Permanent solution, although expensive and riskier.
| Intervention | Price |
| Surgery | $20,000, surgery has risks associated |
This treatment approach becomes an ongoing cost.
| Treatment approach | cost |
| Medical consultation | $200 |
| Sleep study | $500 |
| Cpap machine | $700-1500 every 5-10 years to replace. Stopgap solution |
Cheap solution, free
| Treatment approach | cost |
| Chewing hard foods | Negligible. Lifestyle change, a person would need to eat already. |
Sleep apnea treatment costs across different approaches
Intervention approach -
| Intervention method 1: Mewing | Intervention 2: CPAP | Intervention 3: Braces | Intervention 4: Surgery |
| Aspect & cost: | $20,000 | |||
| $6000 | ||||
| Medical consultation | Optional $200 | $200 | $200 | |
| Sleep study | $500 | $500 | ||
| Cpap machine | $700-1500 every 5-10 years to replace. | |||
| Chewing hard foods | negligible | |||
| Hard gum | Negligible | |||
| Postural checking | Negligible |
Neglectedness
Mewing scores 12 on the neglectedness scale (the highest score).
Is there any reason to expect this problem not to be solved by: (i) markets (ii) government (iii) other individuals looking to have a social impact?
- Markets are incentivised to profit from surgeries more than mewing
- Governments will probably jump on board if the cause can get a little more advocacy
- Yes other individuals will help but a more organised effort is going to be more valuable.
Within research, is this a new field, or at the intersection of two disciplines? These areas are most likely to get neglected by academia.
There are already books supporting this cause area.
If you don’t work on the problem, how likely is it someone else will step in instead?
There seems to be only a few passionate people, fuelling work on the project out of their own spare time and personal investment.
If you work on this problem, will you learn more about how pressing it is compared to other problems?
Probably. Exposure to the problem will continue to show how important it is.
Comments on the Novelty of this situation
- Lack of receptivity from the orthodontic world due to a focus on treating symptoms (crooked teeth) versus looking at evolutionary dentistry patterns and preventing the condition. There’s a belief this is genetic among the dental community or a focus on removing or moving teeth rather than focusing on the jaws themselves. because they will lose money.
- Indeed, environmental influences on skeletal growth are largely ignored by the orthodontic profession, which often accepts jaw skeletal development as genetic in nature, although the teeth themselves are recognized as subject to environmental influences (Proffit 1978, Tulloch et al. 1998, 2004, Dolce et al. 2007, Siara-Olds et al. 2010, Ehsani et al. 2015)
- Dentists are generally positive when they hear about it (What is mewing - https://www.colgate.com/en-us/oral-health/adult-oral-care/what-is-mewing)
- Interesting shape of who’s affected (dependent on food sources, across socioeconomic classes, developed and less developed world)
- It’s surprisingly obvious (feels too good to be true) and that’s the feeling that I should expect for an accidentally unnoticed solution
- Anyone sceptical is freely able to try chewing hard foods and take photos for experimentation.
- Because it doesn’t cost anything to do mewing, it’s a cheap win.
- Because it’s hard to do anything consistently it’s still a public health initiative that requires support (not so easy to shift the culture)
- Encourage “Look into it more”
- Add to public health campaigns
Align with relevant public dental health - like brushing teeth
New EA Cause area - this has the potential to be a new EA cause area, recently uncovered high impact, major health revolution with major solvability and positive available outcomes.
EA Call to action
Public health initiative to solve the problem
- Public health information initiative
- Infographics
- Make some detailed infographics that explain the above.
- Memes
- [make some memes]
- Stickers
- “Are you mewing”
- Posters:
- poster appealing to babies 0-2
- Breastfeeding
- Bottles that mimic the breast
- Shift to foods that are chewy and hard to chew
- poster appealing to young kids 2-10 (for paediatricians, dentists)
- Before and after photos
- Hard foods
- Tongue posture
- Other relevant conditions like adhd, behavioural problems
- Avoid surgery
- Poster appealing to teenagers 10-15
- Before and after photos
- Don’t need braces and permanent dental fixtures
- Beautification of the face
- Avoid surgery
- Breathing improvements
- Attention and focus benefits
- Quality of life improvements
- Sleep quality improvements
- Poster appealing to young adults 16-23
- Before and after photos
- Beautification of the face
- Don’t need braces and permanent dental fixtures
- Mental health benefits
- Sleep quality improvements
- Health improvements
- All round quality of life improvements
- Avoid surgery
- poster appealing to babies 0-2
- Policy
- Infographics
Request from EA
We are proposing that EA take on the initiative to:
- Help us quantify the impact of poor jaw health for EA and global education purposes
- Help spread public information
- Individual effort
- Talk about this and spread the message more
- Self educate - read and watch the simple sources
- Spread Memes
- Spread stickers (contact for stickers to be posted to you)
- Volunteer time towards creating collective effort initiatives
- Collective effort
- Contact various relevant organisations
- Create public health initiatives in every country
- Funding to support the above processes and further research
- Individual effort
We see this as a potential high impact cause area.
Contribute to the cause by getting in touch
For the purpose of this draft being published, you can comment below or email me at redeliot@gmail.com to talk about it.
Return on investment in mewing public information
- Impact on the developed world as well (incredibly rare to be able to help a developed nation)
- Impact on EA people too.
- Neglected nature of the problem
- Fermi cost effectiveness (cost of public information/number of people affected)
Easy to understand resources
- Book: Jaws: The Story of a Hidden Epidemic - Sandra Kahn and Paul ...
- Book: Breath: The New Science of a Lost Art: Nestor, James
- Book: The Story of the Human Body: Evolution, Health, and Disease: Lieberman, Daniel
- Book: Six-Foot Tiger, Three-Foot Cage - Holistic Mouth Solutions
- Paper: The Jaw Epidemic: Recognition, Origins, Cures, and Prevention
- Book: Nutrition and Physical Degeneration - Weston A. Price
- Youtube channel: Orthotropics - YouTube
- Orthodontic practice: Forwardontics
- GOPEX (Good Oral Posture Exercises) book - for parents and kids (5-12)
- Google images search for mewing before and after
- Book: 6.7 Million Wisdom Teeth Removed Unnecessarily Each Year - Cure Tooth Decay
- Article: Why Cavemen Needed No Braces - Stanford University Press Blog.
- Prior EA forum article: New EA cause area: chewier food for children
Scientific references
- Sandra Kahn, Paul Ehrlich, Marcus Feldman, Robert Sapolsky, Simon Wong, The Jaw Epidemic: Recognition, Origins, Cures, and Prevention, BioScience, Volume 70, Issue 9, September 2020, Pages 759–771, https://doi.org/10.1093/biosci/biaa073
- Brunelle JA, Bhat M, Lipton JA. Prevalence and distribution of selected occlusal characteristics in the US population, 1988-1991. J Dent Res. 1996 Feb;75 Spec No:706-13. doi: 10.1177/002203459607502S10. PMID: 8594094.
- Tandon P, Shah S, Dadhich A, Saluja H, Chauhan H. Incidence and Distribution of Jaw Pathologies among 0-15 Years Age Group at a Tertiary Rural Health-Care Center of Maharashtra: A Retrospective Study of 10 Years. Contemp Clin Dent. 2020 Jan-Mar;11(1):39-45. doi: 10.4103/ccd.ccd_328_18. Epub 2020 Jul 13. PMID: 33110307; PMCID: PMC7580751.
- Price, W. A. (2008). Nutrition and Physical Degeneration. United States: Price-Pottenger Nutrition Foundation.
- Young T, Finn L, Peppard PE, Szklo-Coxe M, Austin D, Nieto FJ, Stubbs R, Hla KM. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep. 2008 Aug;31(8):1071-8. PMID: 18714778; PMCID: PMC2542952.
- Lombardo G, Vena F, Negri P, Pagano S, Barilotti C, Paglia L, Colombo S, Orso M, Cianetti S. Worldwide prevalence of malocclusion in the different stages of dentition: A systematic review and meta-analysis. Eur J Paediatr Dent. 2020 Jun;21(2):115-122. doi: 10.23804/ejpd.2020.21.02.05. PMID: 32567942.
Yin H, Yang D, Yang L, Wu G. Relationship between sleep disorders and attention-deficit-hyperactivity disorder in children. Front Pediatr. 2022 Jul 22;10:919572. doi: 10.3389/fped.2022.919572. PMID: 35935380; PMCID: PMC9354977.
https://www.youtube.com/@Orthotropics/videos
https://orthotropics.com/books-and-literature/
https://orthotropics.com/case-studies/
https://80000hours.org/articles/problem-framework/
Nutrition and physical degeneration - weston price (book)
Relevant resources that haven’t been much help when looking for clear statistical citations.
(Around 60% of adults made a dental visit in the previous 12 months and the majority of these visited for a check-up (60%)) https://www.aihw.gov.au/reports/dental-oral-health/adult-oral-health-and-dental-visiting-in-australia/summary
(25.2% Percentage of people reporting that they had felt uncomfortable about their dental appearance ‘very often’, ‘often’ or ‘sometimes’ during the previous 12 months) https://www.aihw.gov.au/reports/dental-oral-health/adult-oral-health-and-dental-visiting-in-australia/summary
(Two-in-five adults (37.8%) reported experiencing financial barriers or hardship associated with dental visiting) https://www.aihw.gov.au/reports/dental-oral-health/adult-oral-health-and-dental-visiting-in-australia/summary
https://www.aihw.gov.au/reports/dental-oral-health/oral-health-and-dental-care-in-australia/contents/costs (Overall, $11.1 billion was spent on dental services in 2020–21)(In 2020–21, per capita expenditure on dental services was $432) (population 25,422,788 - https://www.abs.gov.au/statistics/people/population/population-census/2021)
In 2017–18, around one-third (30%) of adults aged 15 years and over had moderate or severe periodontitis, an increase from around onequarter (23%) in 2004–06. (https://www.aihw.gov.au/reports/dental-oral-health/national-oral-health-plan-2015-2024/contents/our-oral-health-a-national-perspective/periodontitis-prevalence)
1.2: KPI 8 Proportion of people who have avoided eating some foods because of problems with their teeth, mouth or dentures during the last 12 months, by age, states and territories, 2017–18
Proportion of people avoiding eating certain foods during the last 12 months 2017–18 Australia Total 5–14 years 14.4
Proportion of people avoiding eating certain foods during the last 12 months 2017–18 Australia Total 15+ years 23.7
https://www.aihw.gov.au/reports/dental-oral-health/national-oral-health-plan-2015-2024/contents/summary https://www.aihw.gov.au/reports-data/health-conditions-disability-deaths/dental-oral-health/data
“Class I right molar relationship was seen in 57.9% of the children and was generally more frequent in boys… Only 10% of the children aged 9 - 11 years old had an ideal interarch relationship.”
https://pubmed.ncbi.nlm.nih.gov/36687295/
The worldwide prevalence of malocclusion was 56% (95% CI: 11-99), without differences in gender. The highest prevalence was in Africa (81%) and Europe (72%), followed by America (53%) and Asia (48%). https://www.researchgate.net/publication/342393383_Worldwide_prevalence_of_malocclusion_in_the_different_stages_of_dentition_A_systematic_review_and_meta-analysis
Lombardo, Guido & Vena, F & Negri, Paolo & Pagano, Stefano & Barilotti, C & Paglia, L & Colombo, S & Orso, Massimiliano & Cianetti, S. (2020). Worldwide prevalence of malocclusion in the different stages of dentition: A systematic review and meta-analysis. European journal of paediatric dentistry. 21. 115-122. 10.23804/ejpd.2020.21.02.05.
The prevalence of obstructive sleep apnea appears to be perhaps 2%–7% or more in children (Lumeng and Chervin 2008), about 5%–20% in adults in general (Finkel et al. 2009), and over 80% in some elderly populations (Senaratna et al. 2017). The available data have many shortcomings, but a reasonably conservative estimate is that obstructive sleep
The available data have many shortcomings, but a reasonably conservative estimate is that obstructive sleep apnea afflicts at least 1 in 20 people worldwide (Punjabi 2008), which is one indicator of the global extent of the jaw epidemic
{kind=link}
{kind=link}
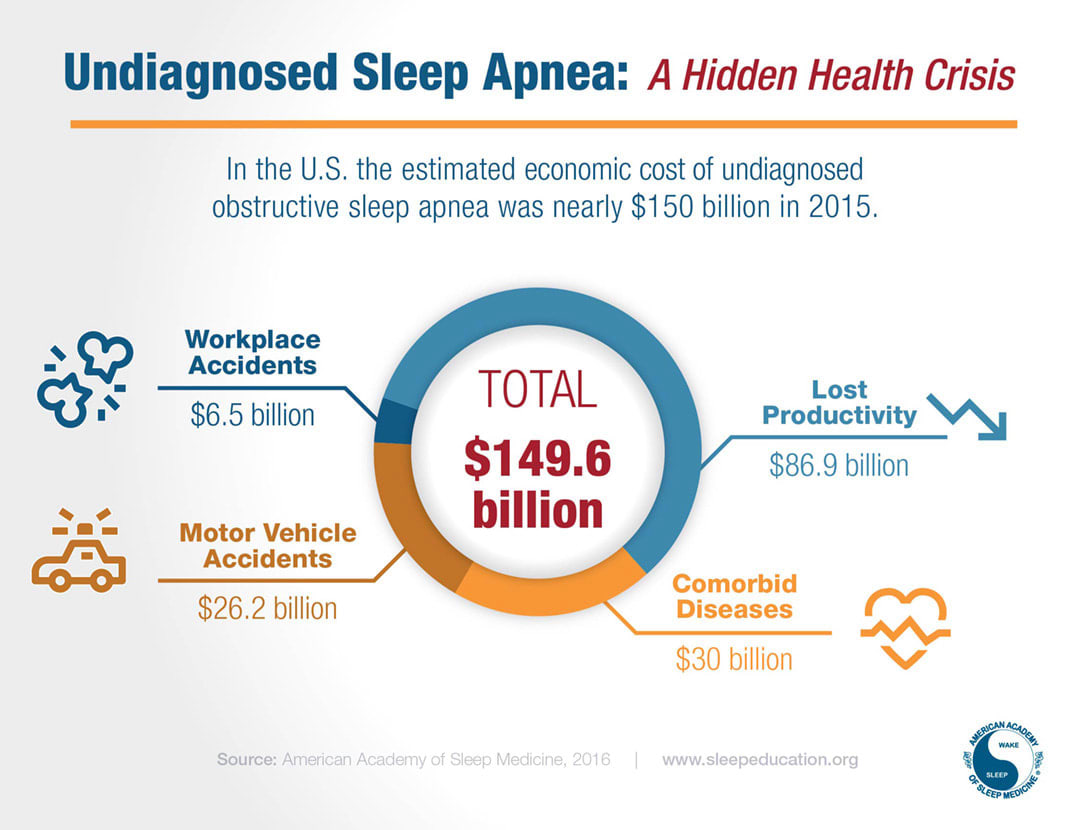
https://aasm.org/economic-burden-of-undiagnosed-sleep-apnea-in-u-s-is-nearly-150b-per-year/
We have found no data on the frequency of UARS, but it seems reasonable to assume that it is higher than the frequency of obstructive sleep apnea.
Agriculture and industrialization encouraged a more sedentary lifestyle, moving indoors, where ventilation rates are low and allergens are concentrated (Bornehag et al. 2005). Subsequent sending offspring to viral sinks, such as daycare centers, and other factors in civilization resulted in developed countries having 20%–25% of children under 5 suffer blockage of the nasal airway in early life (Jesenak et al. 2011). A stuffy nose automatically leads to mouth breathing and reverse swallowing, altering the shape of the jaws and face during development (Jefferson 2010).
https://news.stanford.edu/2020/07/21/toll-shrinking-jaws-human-health/
https://www.smithsonianmag.com/smart-news/how-dawn-farming-changed-our-mouths-worst-180954167/
https://www.allergy.org.au/images/stories/pospapers/2007_economic_impact_allergies_report_13nov.pdf
Observational studies have linked chronic mouth breathing to structural changes of the face. Nasal obstruction due to allergic rhinitis or adenoid hypertrophy (the so-called ‘adenoid facies’) have been associated with a long and narrow face, a long narrow tongue, high arched palate, small lower jaw, over bite and cross bite and dental crowding and malocclusion. Animal studies have demonstrated the development of similar abnormalities in experimental models. Furthermore, some have been shown to be reversible when the obstruction has been relieved.
Don't shoot me it's a draft! Publishing early for the week. I hope this gets read and thought about and talked about.
Credit needs to go to my co-authors too @Tharun Sonti, @SereneDesiree, Evan Hockings, @Chriswaterguy and the many others who have commented along the way. Sorry it's not done but I'd rather get it out there.
The evidence for mewing just doesn’t seem to be there. You give a lot of theory and anecdote and before/after photos, which aren’t worth much. The main proper source I see you list is https://academic.oup.com/bioscience/article/70/9/759/5872832?login=false, which itself seems to admit that there’s a lack of evidence for it
One piece of evidence that feels convincing to me while still being anecdotal is the google images page for "mewing before and after"
https://www.google.com/search?sca_esv=b59cd4dbe0a194eb&sxsrf=AHTn8zon1EAYpPRhYbygOoHRzOeof93GlA:1740266143676&q=mewing+before+and+after&udm=2&fbs=ABzOT_CWdhQLP1FcmU5B0fn3xuWpA-dk4wpBWOGsoR7DG5zJBr1qLlHFB6ZBcx-Arq68_wdJlnBwAHirUEMwdE4O8L3EsOBFudme3Tao3KPzT2BTFK5Z7JuPMxKZBMYVPqa-00-_f9CmdNmTUXzgQ7vPp3ChppYRWHxEMFYTZzrvgqh9i5jkr_SnWZ9F_SmwYzbtLLpQf6bCsYahVhoF5ifkXkrkPY9ZfQ&sa=X&ved=2ahUKEwj4x7vKtNiLAxWgqFYBHbucLFwQtKgLegQIFxAB&biw=1920&bih=953&dpr=1
What you can find is a variety of people's photos in generally self-posted format claiming to have achieved results via mewing.
Some of those may include surgical assistance but I take most of those photos for what they are at face value - mewing produces results.
Do you have an alternative explanation of what's going on there? Why are there all these images that seem to point towards mewing?
What evidence would you need to be convinced that mewing is a fruitful endeavor?
Looking at the hierarchy of evidence - https://en.wikipedia.org/wiki/Hierarchy_of_evidence (https://en.wikipedia.org/wiki/Hierarchy_of_evidence#/media/File:Research_design_and_evidence.svg)
The current evidence sits at 3 or 4 in this list. That's still not randomized controlled trials but those happen to be much harder to run than the prior levels in the pyramid. I see the current evidence as meriting the RCT but maybe you see it differently?
I didn’t see case-control studies or cohort studies. You should link to those.
Before and after photos are prone to manipulation and bias
Take a photo with your jaw pulled back for the before and then one with your jaw projected forward for the after. Use better lighting for after. Even if the person is not consciously intending to, these are so easy to manipulate.
Maybe surgery was done in some of those photos and the poster is not being forthcoming about that, if they have something to sell.
I agree on the "if they have something to sell" but there really isn't much to sell here. Chew hard food, practice better posture and lip tape at night. It's not a financially viable industry to sell in.
Occasionally people sell gum. But they aren't rolling in riches in the process of selling gum.
Sometimes people facilitate accountability groups and there's a finance factor there but it's not very common. And that's a private coaching group, it takes work to maintain.
Yes photos are open to manipulation by lighting and some are like that but I don't think all of them are manipulated.
The cohorts are the studies of countries or societies with access to different diets. Weston price did that in the 1930s and looked at the skull records which are hard to fake (and hard to verify for others trying to validate his work). But it's harder to find recent cohorts with strict diet limits.
I'll try to dig up the case studies although all this work and it's likely you will say that case studies are not convincing without rct's. This is why I never published the draft. It's a lot of work and it's not worth my energy to prove the theory to random people on the internet.
Using different countries as cohorts introduces all sorts of confounding factors.
People will put forward a biased case even without a financial incentive. Maybe a person genuinely believes that the weight-loss or skincare regimen they followed worked, and they want to put the best case forward so other people benefit from it, so they use the worst Before and best After photo to be more convincing. People who saw no difference won’t post at all.
The reason RCTs exist is because time and time again we’ve seen that looking at anecdotes and individual case studies leads to conclusions that turn out to be wrong when you RCT them. Might seem nitpicky but you just end up wrong half the time otherwise.
I agree.
I believe that we need an rct but without subjective wins from the gradually mounting evidence, the whole conversation is me pushing uphill for a cause that I'm only a bit motivated to prove to other people.
I'm confident for myself but the potential cause area needs more research.
I agree there's something here, but I think you're overselling the theory's level of backup. It really lost me at the ADHD part.
My summary from when I looked at this when trying to figure out orthodontics for my kid:
"Orthodontists evaluated Norwegian skulls from 500 years ago and from now. https://pubmed.ncbi.nlm.nih.gov/17561048/ "Only 36% of the medieval group showed objective assessed needs for orthodontic treatment, compared with 65% of the present-day sample." Similar study in China, with a 4000-year-old sample because China. https://pubmed.ncbi.nlm.nih.gov/22340477/"
This made me think that in pre-modern environments, tooth/jaw problems were better but not absent.
Getting kids to do things differently (holding their body differently, eating different foods) seems pretty hard. One more tractable intervention could be informing parents as consumers of orthodontics that there are downsides to making the mouth smaller. E.g. when I talked to different orthodontists, one proposed pulling teeth to reduce teeth crowding, while the others wanted to use an expander to make more room.
Thanks for the write-up :) I agree with the other commenters. In particular, I'm inclined to think it's too early for the suggested actions, especially the proposed public health initiative. I think it would be interesting to see more research, but a public health initiative is premature.
You say:
This makes sense, but by doing more studies on mewing, we may move mewing up the hierarchy of evidence, yet in the process find that the effect is not as large as we might have hoped. Or maybe there are other factors that come into play such as low adherence (as Julia suggested). That is, being in the early adopters phase / being low on the hierarchy of evidence isn't a reason to act with insufficient evidence.
I think there's progress to be made here, but it's at the stage of information-gathering, not a public health initiative (yet).