Summary
Kidney stones cause an immense amount of suffering worldwide. Weighted by their intensity, and depending on some assumptions, we posit that kidney stones may account for a large fraction of human suffering worldwide.[1] Finding cost-effective solutions for this hedonic catastrophe should be a very high priority in any suffering-focused research agenda.
While researching kidney stone pain, we were very impressed with the online reports of patients using chanca piedra (Phyllanthus niruri) to treat their pain and prevent the formation of stones, so we decided to take a closer look. Given the limited number of high-quality studies on the efficacy of chanca piedra, we decided to look for additional evidence online and collected thousands of WebMD, Amazon, and Reddit reviews about chanca piedra and other kidney stone treatments, and classified them along a few dozen different dimensions (such as reported side effects, reported pain reduction, etc.).
While we acknowledge that internet reviews are not usually a reliable source of information concerning medical matters, we also make the case that the reviews of chanca piedra in particular should not be dismissed out of hand. In particular, we find that chanca piedra:
- Is effective for an exceptionally high percentage of people, judging by both the star ratings and review contents.
- Has an exceptionally low rate of reported side effects.
- Has high-quality reviews, judged by criteria such as providing adequate context and believable narratives consistent with kidney stone experiences.
- Is supported by reviews that are equally very positive across WebMD, Amazon, and Reddit.
- Compares very favorably to the WebMD reviews of standard prescription medications for kidney stones, including: tamsulosin (aka Flomax), allopurinol, potassium citrate, and hydrochlorothiazide.
Has a far lower rate of reported side effects and a higher rate of effectiveness than melatonin and ashwagandha, two widely used over-the-counter supplements generally recognized as safe and effective, which we include as a sanity check.[2]
- Is likely an effective prophylactic based on the reviews by those who report to be using it as such. This is perhaps one of the most significant aspects. We get the strong impression that chanca piedra is more effective as a preventative medicine than a source of acute relief. This, along with the unusually low rate of side effects reported, is what motivates us to explore its use in preventative medicine as a possible philanthropic cause area.
We address the epistemological concerns around updating one’s sense of how promising chanca piedra is based on internet reviews, and argue that the most likely reasons for such high ratings possibly being fake do not seem consistent with the whole picture so far. In particular, we argue that:
- These reviews are consistent with the current scientific literature: Stones can indeed dissolve or become smoother [2,3], and patients taking chanca piedra also report exceptionally low rates of side effects [4–6].
- Our observations are inconsistent with astroturfing, primarily because of the general lack of emphasis on specific brands in the reviews and, secondarily, due to the consistency of reviews across brands and methods of consumption.
Selection effects do not seem to be strong enough to explain away these reviews: It is true that both exceptionally good and exceptionally bad responses to a treatment or supplement motivate people to write reviews. That said, this seems inconsistent with the lack of side effects reported. Although selection effects should make us very cautious when interpreting the absolute base-rate of specific effects, contrasting such base-rates across the reviews of various treatments is valuable information that controls (to a large extent) for selection effects.[3]
We also discuss what we can do about this, why chanca piedra does not yet appear on official sites, and how we envision a way for this intervention to significantly reduce extreme pain worldwide.
Following the ITN framework, kidney stones are clearly important due to the scope and severity of the suffering [42]. While it may seem that kidney stones are not a neglected problem, we argue that there is at least an epistemological angle that is neglected. And if we do find cheap solutions that are both medically safe and highly effective at reducing the enormous amount of suffering associated with this condition, the problem also becomes much more tractable.
Context
At the Qualia Research Institute, we advocate for and carry out work on the following three pillars (among others):
- Preventing negative extremes: Finding cost-effective ways to reduce extreme suffering at scale.
- Increasing the baseline: Identifying cost-effective interventions that reliably increase people’s health and hedonic baselines.
- Achieving new heights: Studying the most positive states of consciousness to uncover the underlying mathematical structure for valence whilst gaining safe and sustainable access to such states.
Work on (2) and (3) involves foundational neuroscience research and high-quality phenomenological practice. In contrast, the work involved in (1) largely involves amplifying neglected, tractable, and significant interventions to reduce and prevent intense suffering that are perhaps not currently explored at scale due to misaligned incentives.
Some examples of our work on (1) include[4]:
- Anti-Tolerance Drugs
- Get-Out-Of-Hell-Free Necklace
- Using Ibogaine to Create Friendlier Opioids
- Cluster Headache Frequency Follows a Long-Tail Distribution
Treating Cluster Headaches Using N,N-DMT and Other Tryptamines[5]
- Quantifying the Global Burden of Extreme Pain from Cluster Headaches
- Logarithmic Scales of Pleasure and Pain: Rating, Ranking, and Comparing Peak Experiences Suggest the Existence of Long Tails for Bliss and Suffering
Introduction
If you ever stumble upon an internet thread about “the worst pain you have experienced,” e.g., in Quora (e.g., 1, 2, 3), Reddit (e.g., 4, 5, 6), or elsewhere, the responses typically go like this: The top-voted answer is a very dramatic account—often a freak accident or a rare disease—that strikes the balance between raw horribleness and a quality of “unlikeliness” that makes it easy to consume as a curiosity. The content is gladly coded as “educational” in nature and illuminating for the human condition. But there is a sense of “otherness”: Whatever the weird thing was that happened to that person, it will probably never happen to you or your loved ones. But then, after a few reports (and perhaps some references to romantic heartache, losing family members, or complaints about surgeries gone wrong), one inevitably finds an answer discussing the pain of kidney stones. And, in response to that post, you also typically find many comments such as “same,” “that’s me, exactly,” “I couldn’t have described it better,” and “I wouldn’t wish that pain on my worst enemy.” But, for some reason, what seems to “stick” from these posts is invariably the weird, unlikely events rather than the mundane ones, however bad they may be.
According to a pilot survey (n=28) we ran among kidney stone sufferers, 17/27 (~60%) describe the experience as being “by far the worst pain” in their lives,[6] with such pain usually being present between 10–100 hours per stone.[7] People who have had kidney stones in the past are at a much greater risk of getting more in the future: About 50% of first time stoners get another stone within seven years of the first one [7]. Given the seemingly long-tailed nature of the distribution of kidney stones per person, every kidney stone you have increases the probability that you will have more in the future, with people at the tail end often describing themselves as “stone mills” and, based on reports online (though no study we could find, unfortunately), being at a potentially greater risk of suicide.
In a study looking at the fear of kidney stone recurrence among 100 patients, Richards et al. [8] found that “more than half of patients (51%) reported that they feared their KS [kidney stones] would return, with 25% reporting strong feelings about the KS returning ‘all of the time’ and 43% worrying ‘a lot’ or ‘all of the time’ about their KS recurring.”
Can vouch, the pain is so extreme it is almost like a living thing; a living thing that does not want to kill you, sadly. Oh, no, death is too good for you. This thing is all about the torture. [...] That pain in your side is hard to describe to someone who has never had them. It is pure, unadulterated, undiffused, exquisite pain. (Source)
Scope
The lifetime prevalence of kidney stones is 10–15% in the developed world and as high as 20–25% in the Middle East [9]. The prevalence of kidney stones in the US doubled between ~1970 and ~2005 [10], and the growing trend continues worldwide [11]. As of 2012, 8.8% of the US population had a kidney stone [12]. The yearly incidence in North America and Europe is about 0.5% [9]. In 2005, annual medical costs for kidney stone treatments in the US averaged $3,500 per patient [13]. Kidney stones were responsible for about 1 million emergency department visits in the US in 2009 [14]. In 2015, kidney stones cost the US $10 billion, making it the most expensive urologic condition [15].
Since lifestyle factors and diet are major contributors to the increase in prevalence of kidney stones (such as sugary drink consumption, vitamin C consumption in large doses,[8] [9] or obesity [17]), official sources typically emphasize lifestyle and dietary interventions as the main strategy to prevent kidney stones. However, drinking 3 liters of water per day[10] is not realistic for many, and “eating right” to avoid kidney stones is also not trivial (nor does it guarantee future stone prevention). Plus, since kidney stones are more common in regions with higher temperatures (likely due to dehydration), climate change is expected to further increase the prevalence of kidney stones [17]. Concerningly, official sources and popular health websites often provide contradictory advice.[11]
Overall, these trends and projections paint a pessimistic picture of our ability to win the battle against kidney stones, and likely contribute to a desensitization towards this problem, given its perceived inevitability. A large reduction in kidney stone cases might not seem within reach for the time being. Unless…well, keep reading.
A Thought Experiment
In order to try and see the problem anew, overcome our desensitization, and imagine solutions, let us consider the following hypothetical scenario:
Imagine that, every year, half a million people in the US (and many more worldwide) get kidnapped by a gang known to use red-hot rods to poke holes into people’s abdomens repeatedly for hours every day, causing a pain so intense and unrelenting that more than half of the victims describe it as “by far the worst pain of their entire lives,” more often than not “worse than childbirth,” and the sort of pain that reliably makes you “want to be dead.” The gang does this skilfully, rarely causing lethal casualties (though organ damage is not uncommon [21]). The torture usually consists of 10 to 100 hours of continuous, ultra-intense pain (although for some people the torture might last much longer). After the family pays a ransom of about $3,500 on average (but much more in the worst cases), the person gets released. Sadly, a happy ending is never guaranteed: The probability of being kidnapped again rises with each kidnapping.
This situation has been going on for as long as we can remember, although kidnapping rates have increased substantially in the last few decades, from ~5% to up to 15% in some regions.
Now imagine that you could cut your chances in half by paying a grand total of $5/year with either no or negligible side effects. Would you do it? Would you pay to be insured against this 1-in-200 event that could happen to you and your loved ones at any time now?
Statistically, that would prevent a single kidnapping for $2,000. Is that worth it? Do we break even? Recall that the ransom already costs $3,500 on average. So even just on purely economic grounds (disregarding costs to one’s subjective well-being, long-term health, and reduced productivity), you are already ahead. Is such a thing even possible? This seems too good to be true. What probability of such a claim being true would justify investigating it more deeply? Arguably, the benefit is large enough that even a small probability might warrant further examination.
We argue that we potentially find ourselves in this scenario, but mapped onto the problem of kidney stones.
A Preliminary Case for Chanca Piedra
The idea that chanca piedra would be the equivalent of the $5/year intervention discussed above is the optimistic scenario, but in our current model, not an unrealistic one. Before we make a detailed case for chanca piedra, we would like to offer a high-level argument illustrating our point.
Consider this: A 4.5-star bottle of chanca piedra with 120 pills costs $19. Each pill is 800mg, higher than that of many other seemingly effective versions. A month-long course of chanca piedra can thus cost under $5, easily.
Next, of the 87 WebMD reviews of chanca piedra by users who take it for kidney stones, 86% said it helped either prevent them, pass them more easily, break/shrink/dissolve/soften them, or reduce pain.[12] Notably, only 7% of users reported any side effects, which is remarkable given that 48% of the 271 WebMD reviews of ashwagandha we analyzed mentioned side effects, as well as 50% of the 161 reviews of melatonin. Keep in mind that both ashwagandha and melatonin are widely used, recommended, and considered to have only mild (if any) side effects. Perhaps you, the reader, have even taken them, or you take them on a regular basis. This is one of the key arguments we want to bring forward in this post: While we acknowledge that online reviews are generally not trustworthy, we should still expect to see statistically meaningful differences across products if they actually differ in efficacy and side effect profiles, especially when comparing reviews within the same platform to (largely) account for platform-specific biases.
The reviews we surveyed (more below) are, to us, very encouraging. But why should we expect yearly courses of chanca piedra to be so effective at preventing stones to begin with? We think that, from logic and heuristics alone, and to a first approximation, it is not unreasonable to expect that chanca piedra will be better at preventing stones than at dealing with already-existing large stones.
Here is our reasoning: The percentage of crystals in your kidneys affected by the active compounds in chanca piedra on a given dose is a function of the surface area exposed to it. As a consequence, a single large stone will take much longer to weaken/break/dissolve than ten fragments with an equivalent mass,[13] which in turn will take much longer to dissolve than an equivalent amount of fine powder made of the same material. In brief, the more centralized, compact, and round the stone formations are, the longer they will take to dissolve relative to their overall mass. When one’s kidneys are close to free of such crystals, though, by their nature they will be very tiny. At that stage, the risk will come from having small nucleations form to begin with and then from having them become the nidus for stone growth (including through processes like Randall's plaque and Randall's plug formation [22]). At that stage, the surface area will be very large relative to the mass, and chanca piedra might easily, in a way, “blast the nucleation seeds out of the water”.
As a consequence, a protocol where one takes, e.g., chanca piedra for a week or a month once a year might keep you at a level where stones never even develop to begin with. Removing the nucleation crystals entirely once a year makes the appearance and then growth of stones start from zero each time.[14] So this might be a way for you to stay stone-free all your life. In other words, I think it is likely that staying stone-free might be much easier than becoming stone-free. That said, this is, of course, speculation. But to us, it is plausible enough that the probability of it being the case might deserve a lot of attention.
Importantly, this optimistic scenario can be further improved by the economies of scale. You could get 5kg of chanca piedra powder for $170, which could easily last you a lifetime with this treatment protocol. If everyone did it, we’d be preventing someone from getting the condition at some point in their life for just ~2 x $170 (assuming a 50% success rate). Government-sponsored programs for large-scale cultivation of the plant or, even better, cheap synthesis and subsidization of the active ingredients could both drastically push the cost further down. You get the idea.
Pessimistically, chanca piedra either has many more side effects than we have been led to believe, or one requires a lot more of it in order to (statistically) prevent kidney stone formation. If we needed a pill every day for the rest of our lives, then the cost would rise to about $60 a year (three bottles of 120 pills, each for ~$20), and with a (very) pessimistic 10% reduction in the probability of developing kidney stones with this treatment, the cost would rise to about $60 x 300 x 10 = $180,000. In this case, the economic case would almost certainly not work out. That said, we strongly suspect that the reality is much closer to the optimistic scenario than the pessimistic one. Importantly, even if chanca piedra does not prevent kidney stones entirely, it will most likely reduce their severity significantly. So, the pessimistic scenario is, we think, rather unlikely.
Chanca Piedra as an Acute and Prophylactic Treatment
In this section, we discuss the existing literature on the use of chanca piedra to prevent and treat kidney stones. We also briefly discuss current treatment options and a few alternative treatments that haven’t been studied much yet. We then present the results of our analysis of thousands of WebMD, Amazon, and Reddit reviews of chanca piedra and other products for kidney stones. Finally, we mention a few cost-benefit considerations.
Randomized Controlled Trials
To our knowledge, only two RCTs exist that look at the effectiveness of chanca piedra to treat kidney stones, with the last one being published 20 years ago.
Nishiura et al. [24] looked at the effects of chanca piedra on urinary biochemistry in 69 patients with calcium stones. Patients were randomized to take either chanca piedra (n=33, 450 mg capsules 3x/day) or placebo (n=36) for 3 months. The study found significantly reduced urinary calcium levels, which is a major risk factor for kidney stones. However, no significant differences were found in the number of stones, the size of the stones, the rate of stone passage, or pain relief. The authors note that since the study “was not intended to identify the differences in clinical characteristics, we believe that the short-term nature of our observations and the relatively small number of patients might have accounted for these negative findings.” They also suggest that the dosage might have been too low.
Micali et al. [5] looked at 150 patients with calcium oxalate kidney stones who all received 1–3 sessions of extracorporeal shock wave lithotripsy (ESWL). After treatment, 78 patients were given a chanca piedra extract (2g daily) for at least 3 months (group 1), while 72 patients served as controls (group 2). Stone clearance was assessed using abdominal x-ray and ultrasound at 30, 60, 90, and 180 days, with "stone-free" defined as either having no stones or only residual fragments smaller than 3mm. They found that “stone-free rate […] was 93.5% in group 1 and 83.3% in group 2 (p=0.48) at the end point of the followup (180 days). For lower caliceal stones (56 patients), the stone-free rate was 93.7% in the treatment group and 70.8% in the control group (p=0.01). Re-treatment needed for group 1 was 39.7%, and for group 2 it was 43.3% (p=0.2). No side effects were recorded with extracorporeal shock wave lithotripsy or P. niruri therapy.” They concluded that “regular self-administration of P. niruri after extracorporeal shock wave lithotripsy for renal stones results in an increased stone-free rate that appears statistically significant for lower caliceal location. Its efficacy and the absolute lack of side effects make this therapy suitable to improve overall outcomes after extracorporeal shock wave lithotripsy for lower pole stones.”
Other Notable Studies
Campos & Schor [25] studied the effects of different concentrations of chanca piedra extract on kidney cells in lab dishes that were exposed to calcium oxalate crystals (the main component of many kidney stones). They found that the extract strongly prevented kidney cells from absorbing the crystals, even with very low concentrations of extract and high concentrations of crystals. The extract wasn’t toxic to the cells even at high doses, leading the authors to suggest that it “may represent a nontoxic, low-cost, and bioavailable therapeutic alternative for the management of urolithiasis.”
A single-arm study by Pucci et al. [6] followed 56 kidney stone patients who took chanca piedra tea for 12 weeks (2 x 250mL of tea infused with 4.5g of dry extract each per day, on alternate weeks), followed by a 12-week “washout” period of no tea. Comparing baseline to post-treatment, stones decreased from 3.2±2.0 to 2.0±2.1 per patient (p=0.0005), urinary oxalate in hyperoxaluric patients decreased from 59.0±11.7 to 28.8±16.0 mg/24h (p=0.0002), and urinary uric acid in hyperuricosuric patients decreased from 0.77±0.22 to 0.54±0.07 mg/24h (p=0.0057). The researchers concluded that chanca piedra tea was safe and effective for reducing kidney stones, particularly in patients with hyperoxaluria or hyperuricosuria, though they noted that larger clinical studies are needed to validate its use in practice.
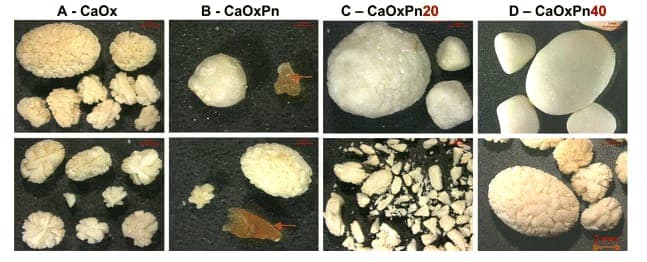
Barros et al. [3] studied how chanca piedra extract affects the formation of calcium oxalate crystals in lab conditions using human and rat urine samples. They added sodium oxalate to trigger crystal formation with and without the plant extract (0.25 mg/mL) present and analyzed the resulting crystals immediately and after 24 hours. While the extract didn't prevent crystal formation, it produced significantly smaller crystals, increased the proportion of less-harmful dihydrate crystals, and prevented crystal clumping. The effects were only seen in human urine samples, not in rat urine, suggesting that chanca piedra might help prevent kidney stones by interfering with multiple steps of stone formation rather than by stopping crystallization entirely.
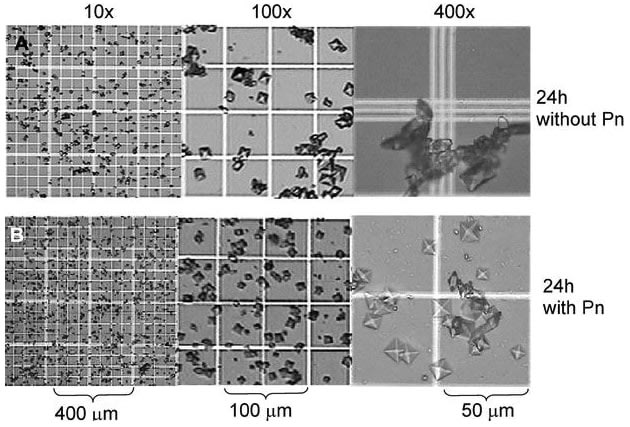
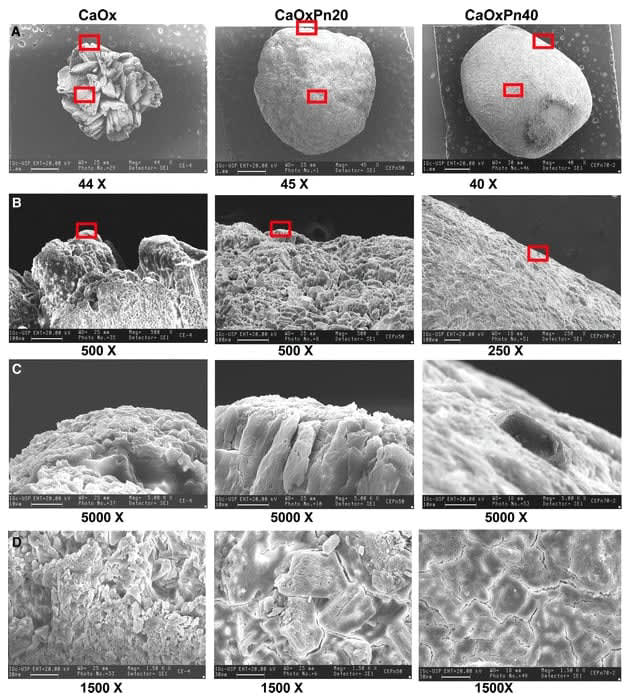
Barros et al. [2] studied the effects of chanca piedra extract on bladder stones in rats by surgically implanting calcium oxalate “seeds” in their bladders. When chanca piedra was given immediately after seeding, it significantly reduced stone formation by 75% in number and 65% in weight (p<0.05). When given after stones had already formed (30 days after seeding), chanca piedra didn't prevent further stone growth; rather, it dramatically altered stone morphology from spiky to smooth surfaces, as confirmed by scanning electron microscopy. The researchers concluded that chanca piedra showed promise both as a preventive treatment and as a potential therapy for existing stones by making them smoother and potentially more fragile, though they noted the need for further evaluation in human patients.[15]
Treatment Options
We reviewed the scientific literature, major health advice websites, and the recommendations of the American Urological Association (AUA) and the European Association of Urology (EAU) to understand what treatments are currently recommended to treat kidney stones (excluding lifestyle and dietary recommendations).
The most commonly recommended pharmacologic interventions are[16]:
| Intervention | Description | AUA Recommendation | EAU Recommendation |
| Thiazide diuretics (e.g., hydrochlorothiazide) | They decrease the risk of calcium stone formation by reducing urinary calcium excretion. | Standard (Grade B) | Strong |
| Potassium citrate | An alkalinizing agent that increases urinary pH and citrate levels, inhibiting calcium crystal formation and preventing stone formation. | Standard (Grade B) | Strong |
| Allopurinol | It prevents uric acid stone formation by inhibiting xanthine oxidase, which reduces uric acid production and urinary uric acid excretion. | Standard (Grade B) | Strong |
| Tamsulosin (aka Flomax) | An alpha blocker that relaxes the smooth muscle of the urinary passage, easing stone movement. | N/A | Strong (for distal ureteral stones >5mm) |
And in terms of common surgical[17] interventions, we found:
| Intervention | Description | AUA Recommendation | EAU Recommendation |
| Shock Wave Lithotripsy (SWL) | External focused shock waves that pass through the body to break stones into small, passable fragments. | Strong (Grade B) for stones <2cm | N/A |
| Ureteroscopy | Insertion of a thin telescope through natural urinary passages to reach and laser-fragment stones. | Strong (Grade B) for ureteral stones | N/A |
| Percutaneous Nephrolithotomy | Direct access to kidney stones through a small back incision using scopes and instruments to fragment and remove stones. | Strong (Grade C) for stones >2cm | N/A |
Alternative treatments
We have spent many hours reading papers, browsing online fora, and watching videos about chanca piedra, and have kept track of a few interventions that warrant further attention.
Two that come up quite often in online discussions that seem particularly promising to us (which deserve a whole review, literature, survey, etc., analysis of their own) are[18] Phosfood and Rowatinex. Two more that came up occasionally are black seed and garcinia (aka hydroxycitric acid).
The 2024 paper “Systematic review of pharmacological, complementary and alternative therapies for the prevention of calcium oxalate stones” by Lo et al. [27] reviewed 38 studies investigating non-guideline treatments for preventing calcium oxalate kidney stones, including medications, herbal supplements, food and macronutrients, micronutrients, and enzymes and probiotics. They concluded that[19]:
- Tolvaptan, cranberry juice, magnesium citrate, ALLN-177, and malic acid had evidence to reduce urinary risk factors;
- SGLT2i, eicosapentaenoic acid, ethane-1-hydroxy-1, and 1-disphosphonate had evidence to reduce stone formation; and
- Chanca piedra, rice bran, and magnesium hydroxide had evidence of both.
Finally, a few other methods that online sources report as having potential benefits include:
- Riding roller coasters
- “Jump and Bump” method (demonstrated here)
- Jumping on a trampoline
- Mechanized exercise
- Marshmallow root
- Horsetail tea
- Black radish
A Note on Epistemology
The epistemological gold standard in medicine is randomized controlled trials (RCTs) [28]. However, if you subscribe to this too religiously and refuse to look at evidence in other formats, perhaps there is no point in continuing to read (instead, it will suffice to list all the available studies to date, their outcomes, the meta-analyses, and then leaving it at that). This approach can be justified quite easily, after all. There are countless dubious or outright deceptive remedies for kidney stones.[20] Perhaps less extreme, but far more widespread, is the presence of countless untested kidney stone herbal remedies out there. So adopting a mindset of “protecting vulnerable populations from exploitation by dubious alternative medicines” is 100% understandable in this context.
However, we are faced with a bootstrapping problem: If we only accept RCT evidence, but won't conduct RCTs without prior evidence, how do new treatments ever get studied?[21] There has to be a gradient—a sort of ramp up. Perhaps if online reviews of an intervention are great, then it deserves surveys, and then large studies.
We believe there are a few (understandable!) reasons why chanca piedra hasn’t yet been promoted to people’s attention, such as:
Incentive misalignment: Since the raw herb cannot be patented,[22] there is little financial incentive for pharmaceutical companies to fund expensive clinical trials.
- Search engine filters: Google's "Your Money or Your Life" policies prioritize official medical sources for health-related searches—very helpful in general, but it will also prevent the bottom-up surfacing of actually effective methods.
- Attribution challenges: Since kidney stone pain is cyclical in nature (it comes in waves and can stop suddenly), it is difficult to establish the efficacy of a given treatment. Any remedy taken shortly before natural pain relief could be mistakenly credited as effective. However, this confounding factor can be partially mitigated by focusing on reviews from experienced patients who have had multiple kidney stone episodes, as they can compare outcomes across different scenarios and better distinguish genuine treatment effects from coincidental timing.
Despite these challenges, we argue that online reviews of chanca piedra are an overlooked source of evidence that warrant additional scientific studies. Here, all of the caveats will apply, of course. Online reviews about the medical merits of a supplement are generally thought of as unreliable, and the reasons for this include how they can (1) be faked for commercial gain (such as “astroturfing”), (2) be the subject of placebo, (3) be heavily affected by selection effects, (4) draw from skewed populations, (5) include people who don’t suffer from the disease, to name a few.
Despite these caveats, we believe that the reviews for chanca piedra are legitimately impressive enough for a number of reasons, such that the above concerns, while valid, seem insufficient to dismiss the potential of this supplement to become a first-line treatment. The very low rate of side effects and its reported prophylactic effects are particularly noteworthy and might promote it to being considered for mass adoption, even by people who are just “at risk” of kidney stones. Perhaps everyone should take it once a week just in case.
Analysis of Online Reviews
An overview of our main results can be found in this dashboard.[23]
WebMD Reviews
We scraped the WebMD reviews of various products used for kidney stones, namely, allopurinol (13), chanca piedra (87), Flomax (22), hydrochlorothiazide (20), and potassium citrate (24), and classified them across a few dozen dimensions.[24] Additionally, we analyzed the ratings and side effects mentioned for black seed (77) and garcinia (892), but none of the reviews mentioned using the products for kidney stones. Finally, we also analyzed the ratings and side effects mentioned for two popular over-the-counter supplements, namely melatonin (161) and ashwagandha (271). 67% of the kidney stone-specific product reviews were classified manually, and the rest by using an LLM. All other products (specifically, their side effects) were extracted using an LLM.
Our main finding was that 86% of reviewers mentioned chanca piedra helping in some way or another with kidney stones, yet only 7% mentioned any side effects. Table 1 shows the results for all kidney stone products.
Looking at the percentage of reviews reporting any negative side effects, we found for the remaining products: black seed (26%), garcinia (49%), melatonin (30%), and ashwagandha (48%). The overall rating of those four products was: black seed (4.1, 85 reviews), garcinia (2.7, 963 reviews), melatonin (3.8, 417 reviews), and ashwagandha (3.6, 289 reviews).
Chanca piedra also outperformed other kidney stone products along some particularly important dimensions, such as overall pain reduction, breaking/shrinking/softening/dissolution of stones, and painless stone passage (see dashboard).
Interestingly, only 10% of chanca piedra reviews explicitly mentioned using it as a prophylactic (most people reported using it acutely), but all reported it helping. For the remaining products, we found: allopurinol (39%), Flomax (0%), hydrochlorothiazide (30%), and potassium citrate (38%).
| Allopurinol | Chanca piedra | Flomax | HCTZ | Potassium citrate | |
| Total Reviews | 13 (0) | 87 (14) | 22 (1) | 20 (3) | 24 (0) |
| Helps overall with kidney stones | |||||
| Yes | 38% | 86% (93%) | 9% (0%) | 35% (67%) | 42% |
| No | 8% | 3% (0%) | 23% (0%) | 30% (0%) | 8% |
| No information | 54% | 11% (7%) | 68% (100%) | 35% (33%) | 50% |
| Side effects mentioned | |||||
| Yes | 54% | 7% (14%) | 91% (100%) | 65% (33%) | 63% |
Table 1: Kidney stone effectiveness and side effect rates of WebMD reviews. (Numbers in brackets represent very high-quality reviews only.)
Finally, since we were impressed by the overall rating of chanca piedra on WebMD (4.6/5.0), we also scraped the overall rating of all 1,298 vitamins and supplements on the WebMD database. We found that:
- For products with at least 10 reviews, chanca piedra ranked #17 out of 426 (96.2th percentile).
- For products with at least 50 reviews, chanca piedra ranked #5 out of 125 (96.8th percentile).
For products with at least 100 reviews, chanca piedra ranked #2 out of 51 (98.0th percentile).[25]
Amazon Reviews
Next, we scraped and classified 1,456 Amazon reviews of four products used for kidney stones, namely chanca piedra (1,193 reviews[26] across 9 different brands), Phosfood (40 reviews, single proprietary brand), Rowatinex (90 reviews, single proprietary brand), and potassium citrate (133 reviews across 8 brands). All of these reviews explicitly mentioned “stone”. We again classified them along multiple dimensions.[27] 20% of reviews were classified manually and the remaining 80% using an LLM.
Perhaps not surprisingly, the results were much more positive across the board compared to WebMD reviews. Table 2 summarizes the fraction of reviews mentioning the product helping with kidney stones in some way, as well as any negative side effects.
The discrepancy in the rate of side effects of potassium citrate compared to WebMD reviews is particularly striking. Overall, Rowatinex seems to outperform the other three products along the most relevant dimensions, though not by a large margin.
| Chanca piedra | Phosfood | Potassium citrate | Rowatinex | |
| Total Reviews | 1,193 (160) | 40 (3) | 133 (35) | 90 (17) |
| Helps overall with kidney stones | ||||
| Yes | 72% (80%) | 75% (33%) | 91% (94%) | 91% (100%) |
| No | 11% (5%) | 10% (0%) | 0% (0%) | 2% (0%) |
| No information | 17% (15%) | 15% (67%) | 9% (6%) | 7% (0%) |
| Side effects mentioned | ||||
| Yes | 3% (4%) | 8% (0%) | 2% (3%) | 2% (12%) |
Table 2: Kidney stone effectiveness and side effect rates of Amazon reviews. (Numbers in brackets represent very high-quality reviews only.)
Reddit Reviews
Finally, we scraped 2,308 posts and comments in r/KidneyStones mentioning the following products: allopurinol (49), black seed (17), chanca piedra (492), Flomax (1,134), garcinia (38), hydrochlorothiazide (46), Phosfood (2), potassium citrate (509), and Rowatinex (21).[28] Importantly, keep in mind that these are not necessarily product reviews per se, but simply posts and comments mentioning these products (often just in passing, without any judgment). We classified them all using an LLM.[29]
Table 3 summarizes the fraction of posts mentioning the product helping with kidney stones in some way, as well as any negative side effects.
| Allopurinol | Black seed | Chanca piedra | Flomax | Garcinia | Hydrochlorothiazide | Phosfood | Potassium citrate | Rowatinex | |
| Total Reviews | 49 (23) | 17 (5) | 492 (154) | 1134 (489) | 38 (7) | 46 (7) | 2 (0) | 509 (235) | 21 (6) |
| Helps overall with kidney stones | |||||||||
| Yes | 20% (26%) | 24% (40%) | 35% (45%) | 25% (26%) | 42% (29%) | 33% (14%) | 100% | 22% (28%) | 24% (50%) |
| No | 2% (4%) | 6% (0%) | 10% (11%) | 12% (13%) | 0% (0%) | 4% (0%) | 0% | 9% (11%) | 19% (17%) |
| No information | 78% (70%) | 71% (60%) | 55% (44%) | 64% (61%) | 58% (71%) | 63% (86%) | 0% | 69% (61%) | 57% (33%) |
| Side effects mentioned | |||||||||
| Yes | 12% (9%) | 0% (0%) | 7% (11%) | 22% (21%) | 13% (43%) | 9% (14%) | 0% | 13% (15%) | 14% (0%) |
Table 3: Kidney stone effectiveness and side effect rates of Reddit posts. (Numbers in brackets represent very high-quality reviews only.)
Garcinia was positively reviewed particularly by long-term patients, but it has perhaps the worst side effect profile of all the treatments we analyzed.
Our overall assessment of the WebMD, Amazon, and Reddit data is that chanca piedra is at the very least as effective as other commonly-prescribed treatments for kidney stones. The data from very high-quality reviews, as well as from long-term patients or patients who have passed many stones, is even more compelling (see dashboard).
Side Effects
Based on the studies and online reviews, our sense is that chanca piedra is exceptionally well-tolerated.[30] We even found a report of patients who were administered very high doses of an aqueous extract of chanca piedra (>15g/day for 3 months) with no evidence of side effects [25,30]. Our data shows it has fewer side effects than even ashwagandha and melatonin.[31]
Obviously, since the pain caused by kidney stones is so huge, side effects may pale in comparison and so are often not even brought up.
The big picture, as we intuitively gather it, looks like this: Chanca piedra has remarkably few side effects for the majority of people, but it may have some serious side effects for a minority of users. In particular:
Ménière’s disease related to loose crystals in the ears (mentioned by just one person[32]).
- Near-fatal gallbladder swelling after chanca piedra allegedly broke a gallstone (mentioned by just one person).
Kick-starting the process of lots of stones evacuating (for “stone mills” to be weary of; mentioned by just one person, who combined chanca piedra with a mix of apple cider vinegar, turmeric, and honey[33]).
- Dissolving other calcium crystals in the body that we may not even know matter (or are aware of at all).
However, for all of the other products except Rowatinex, we were able to find some reports of severe side effects, such as staph infections from allopurinol, symptoms of transient ischemic attacks from black seed, severe headaches/migraines and fainting from Flomax, serotonin syndrome from garcinia (in combination with antidepressants), fainting from hydrochlorothiazide, tooth damage from Phosfood, irregular heartbeat from potassium citrate, suicidal thoughts from ashwagandha, and rectal bleeding from melatonin. Remember that Side Effects May Include Anything.
On the whole, though, we get the picture of a supplement that has a far smaller rate of side effects than most other supplements and prescription drugs—one that really works.
Cost-Benefit Considerations
Rather than a comprehensive assessment, here we simply want to strengthen the case for chanca piedra based on simple cost-benefit considerations.
In 2011, Lotan & Pearle [26] developed a statistical model to estimate whether a prevention strategy for kidney stones would be cost effective under various assumptions. They concluded that preventive strategies would be cost effective in scenarios where the incidence of stones was at least 1%, the annual cost of prevention did not exceed $20 per person, and the prevention strategy prevented at least 50% of stone cases.[34]
What fraction of stone cases can be prevented with chanca piedra should therefore be a top research priority. Also, as we discussed earlier, since a lifetime supply of chanca piedra could easily be much cheaper than $20/year, the case is strengthened. Implementation costs (lobbying, educational campaigns, distribution, etc.) should also be estimated.
Importantly, these estimates only take into account legible direct economic costs. A far more complete analysis (which, in our opinion, actually addresses the more significant, real cost of kidney stones) would be in terms of subjective well-being, taking into account the acute and long-term suffering caused by this condition. We shouldn’t merely ask ourselves “would I be willing to pay $20/year to save myself the costs of surgery, doctor visits, etc., if I ever get a kidney stone?”, but also to spare ourselves from potentially the worst possible pain we’ll ever experience, with the ensuing stress and anxiety.
Acutely, QALYs and DALYs would be a very poor estimate of the actual cost for the simple reason that they currently do not take into account the logarithmic scales of pain [33,34]. Instead, we should perhaps look into innovative frameworks like the “Hell-Index,” where the (dis)value that one tries to minimize is along the lines of “a country’s yearly total of people-seconds in pain and suffering that are at or above 20 in the McGill Pain Index (or equivalent).”[35]
If we were to rank interventions according to that metric, we posit that preemptive chanca piedra might very well be among the top contenders.
Recommendations
What practical measures do we advocate based on the evidence we’ve presented? Two priorities stand out:
- Consider using chanca piedra as an add-on, following a “More Dakka” approach.
- Increase the notoriety of chanca piedra online so that it reaches as many sufferers as possible.
More Dakka: Chanca Piedra as an Add-On
From More Dakka by Zvi (see also More Dakka in Medicine by Sarah Constantin):
In a MetaMed case, a patient suffered from a disease with a well-known reliable biomarker and a safe treatment. In studies, the treatment improved the biomarker linearly with dosage. Studies observed that sick patients whose biomarkers reached healthy levels experienced full remission. The treatment was fully safe. No one tried increasing the dose enough to reduce the biomarker to healthy levels. If they did, they never reported their results.
We strongly feel that something like this is largely the case with chanca piedra right now. The hundreds of online reviews we reviewed all seemed quite cautious about dose. Yet, nobody reported trying higher doses than prescribed, even when the dose they took seemed to help and they had no side effects (which was most of the time). The typical dose we see in supplements ranges from 200mg all the way up to 3200mg, and we don’t notice any obvious increase in side effects at the upper range (though we have not rigorously quantified this relationship, so please take this with a grain of salt[36]).
Besides merely taking higher doses until we see what kind of effectiveness we can reach and determine when side effects finally manifest in a significant fraction of patients, there are other ways in which we can apply a More Dakka mindset to the problem.
For example, lithotripsy[37] has a 70–90% success rate [37,38] and costs about $3,500 per person [13]. We already have evidence that taking chanca piedra after lithotripsy helps [5]. Would it be possible to boost this success rate further by taking chanca piedra for a few days before the procedure in order to weaken the stones?
Similarly, the EAU states that combining tamsulosin with chemolysis for uric acid stones >8mm in particular is more effective than each treatment alone. And a 2024 study by Mauro et al. [39] showed that a combination of tamsulosin with three herbal extracts (boldine, chanca piedra, and Ononis spinosa) was significantly more effective than tamsulosin alone in treating kidney stones.
Why stop there? If kidney stones are indeed this dire ethical emergency to the sufferer (as we argue it is), wouldn’t trying further stacks of treatments and approaches be worth the marginal, so-far-from-what-we-can-tell risk(s) of doing so?
Obvious More Dakka moves: Combine with Rowatinex, horse tail, marshmallow root, daily coffee, lemon juice, long walks, roller coasters, etc. Obviously More Dakka is obvious.
Increase the Notoriety of Chanca Piedra
Currently, it is not easy for kidney stone sufferers to learn about chanca piedra (and its minimal side effects) via the usual search strategies:
- None of the (at least) top 10, authoritative-looking results when Googling “kidney stones” mention chanca piedra.
- When googling “kidney stone prevention,” only one of the (at least) first 20 results mentions chanca piedra in passing (adding “Use herbal remedies with caution. They’re not well-regulated or well-researched for the prevention or treatment of kidney stones.”)
- The Wikipedia entry about kidney stones does not mention chanca piedra even once.
- The Wikipedia entry about chanca piedra does not mention its use for kidney stones.
- None of the (at least) top 20 search results we get on YouTube when searching “how to prevent kidney stones” mention chanca piedra.
- None of the first few dozen results for “chanca piedra” on YouTube look official or authoritative. They are by and large unserious videos that would put off any scientifically-minded onlooker.
We acknowledge that it’s somewhat intractable to affect the Google search results (unless of course we find ways to update the existing top results) and, to a lesser extent, the YouTube results (unless of course an influencer creates high-quality content on the topic). However, updating the relevant Wikipedia entries could still be tractable.
Also, since chanca piedra is also not endorsed by urological associations, most doctors will likely never suggest it to patients. Perhaps the primary way to overcome this barrier would be to finally have large-scale RCTs testing the efficacy of chanca piedra, and advocating for updates to official urological guidelines.
Final Recommendations
Finally, we suggest:
- Carrying out larger studies on the safety and efficacy of chanca piedra for preventing kidney and gallbladder stones in general populations using several dose regimens and protocols (placebo, 100mg once a day for a month each year, 100mg once a week, 800mg once a week, 800mg once a day).
- Carrying out studies on the safety and effectiveness of increasingly high doses of a combination of chanca piedra and other treatments such as Rowatinex, Phosfood, and potassium citrate, i.e., adopting a More Dakka angle.
- Carrying out large-scale surveys of kidney stone patients to better understand which treatments and products work best, and develop a global ranking.
Investigating the incidence of kidney stones in non-human animals.[38]
- Developing cheaper, more accessible, and more accurate methods for early detection of stones [43].
Cautiously considering taking chanca piedra as a prophylactic yourself (especially if there is a history of kidney stones in your family) or as an acute treatment if you already have kidney stones.[39]
If our estimates are correct that there really is a significant probability that chanca piedra works for, say, effectively preventing kidney stones in 50% of people with minimal side effects, we could be facing the promise of a major hedonic improvement to the human condition, on the scale of millions of people not having to experience intense, hellish pain every year. Validating these preliminary but promising findings could represent one of the most cost-effective ways to reduce extreme suffering at scale.
Author Contributions and Acknowledgements
The original investigation of chanca piedra as a potential high-impact intervention was conceived by Andrés Gómez Emilsson, who developed the core theoretical frameworks including the surface area to mass ratio analysis explaining prophylactic efficacy, the analysis of nucleation prevention versus treatment of formed stones, and a novel epistemological approach to evaluating internet reviews through systematic cross-comparison. He also contributed to the manual classification of hundreds of reviews and wrote the initial draft connecting this work to broader questions of reducing extreme suffering. Alfredo Parra developed these concepts into their final form, adding comprehensive literature review, systematic treatment comparisons, data scraping, LLM classification, data dashboard development, statistical analysis of review data, and final manuscript preparation.
We are particularly grateful to Adam Davis and Aatu Koskensilta for their extensive contributions to WebMD data scraping and classification, thoughtful methodological discussions, and helpful feedback throughout the project, with Adam Davis also providing additional manual review classification and final manuscript review and proofreading. Andrew Zuckerman provided valuable early methodological guidance on review analysis approaches.
We also deeply thank Hunter Meyer, Sean McGowan, and Tyler Strause-Tabares for their technical support throughout various stages of the project. Special acknowledgement goes to Dan Elton for their EA Forum essay "Kidney stone pain as a potential cause area," which helped validate this research direction, and to the Qualia Research Institute for providing the institutional framework supporting novel research into overlooked opportunities for reducing suffering.
Finally, we are profoundly grateful to our donors and supporters who make this work possible,[40] and to the broader effective altruism community for fostering an environment where unconventional but potentially high-impact research directions can be pursued in service of doing the most good possible with limited resources.
References
1. Miah, S. et al. Renal colic and childbirth pain: female experience versus male perception. J. Pain Res. 10, 1553–1554 (2017).
2. Barros, M. E. et al. Effect of extract of Phyllanthus niruri on crystal deposition in experimental urolithiasis. Urol. Res. 34, 351–357 (2006).
3. Barros, M. E., Schor, N. & Boim, M. A. Effects of an aqueous extract from Phyllantus niruri on calcium oxalate crystallization in vitro. Urol. Res. 30, 374–379 (2003).
4. Boim, M. A., Heilberg, I. P. & Schor, N. Phyllanthus niruri as a promising alternative treatment for nephrolithiasis. Int. Braz J Urol Off. J. Braz. Soc. Urol. 36, 657–664; discussion 664 (2010).
5. Micali, S. et al. Can Phyllanthus niruri affect the efficacy of extracorporeal shock wave lithotripsy for renal stones? A randomized, prospective, long-term study. J. Urol. 176, 1020–1022 (2006).
6. Pucci, N. D. et al. Effect of phyllanthus niruri on metabolic parameters of patients with kidney stone: a perspective for disease prevention. Int. Braz. J. Urol. 44, 758–764 (2018).
7. LeWine, H. E. How to prevent kidney stones. Harv. Health (2023). At <https://www.health.harvard.edu/blog/5-steps-for-preventing-kidney-stones-201310046721>
8. Richards, H. L., Fortune, D. G. & Hennessey, D. Fear of kidney stone recurrence – an unexamined factor in patients with kidney stones. Eur. Urol. Open Sci. 67, S29 (2024).
9. Kidney stone disease. Wikipedia (2025). At <https://en.wikipedia.org/wiki/Kidney_stone_disease#Epidemiology>
10. Romero, V., Akpinar, H. & Assimos, D. G. Kidney stones: A global picture of prevalence, incidence, and associated risk factors. Rev. Urol. 12, e86–e96 (2010).
11. Sorokin, I. et al. Epidemiology of stone disease across the world. World J. Urol. 35, 1301–1320 (2017).
12. Scales, C. D., Smith, A. C., Hanley, J. M. & Saigal, C. S. Prevalence of kidney stones in the United States. Eur. Urol. 62, 160–165 (2012).
13. Saigal, C. S., Joyce, G., Timilsina, A. R., & the Urologic Diseases in America Project. Direct and indirect costs of nephrolithiasis in an employed population: Opportunity for disease management? Kidney Int. 68, 1808–1814 (2005).
14. Fwu, C.-W., Eggers, P. W., Kimmel, P. L., Kusek, J. W. & Kirkali, Z. Emergency department visits, use of imaging, and drugs for urolithiasis have increased in the United States. Kidney Int. 83, 479–486 (2013).
15. Kirkali, Z., Rasooly, R., Star, R. A. & Rodgers, G. P. Urinary stone disease: Progress, status, and needs. Urology 86, 651–653 (2015).
16. Thomas, L. D. K., Elinder, C.-G., Tiselius, H.-G., Wolk, A. & Åkesson, A. Ascorbic acid supplements and kidney stone incidence among men: A prospective study. JAMA Intern. Med. 173, 386–388 (2013).
17. Stamatelou, K. & Goldfarb, D. S. Epidemiology of kidney stones. Healthcare 11, 424 (2023).
18. Xu, C. et al. Self-fluid management in prevention of kidney stones: A PRISMA-compliant systematic review and dose–response meta-analysis of observational studies. Medicine (Baltimore) 94, e1042 (2015).
19. Peerapen, P. & Thongboonkerd, V. Kidney stone prevention. Adv. Nutr. 14, 555–569 (2023).
20. Ferraro, P. M. & Curhan, G. C. More good news: Coffee prevents kidney stones. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 79, 3–4 (2022).
21. Tang, X. & Lieske, J. C. Acute and chronic kidney injury in nephrolithiasis. Curr. Opin. Nephrol. Hypertens. 23, 385–390 (2014).
22. Khan, S. R. & Canales, B. K. A unified theory on the pathogenesis of Randall’s plaques and plugs. Urolithiasis 43, 109–123 (2015).
23. Bird, V. Y. & Khan, S. R. How do stones form? Is unification of theories on stone formation possible? Arch. Esp. Urol. 70, 12–27 (2017).
24. Nishiura, J. L., Campos, A. H., Boim, M. A., Heilberg, I. P. & Schor, N. Phyllanthus niruri normalizes elevated urinary calcium levels in calcium stone forming (CSF) patients. Urol. Res. 32, 362–366 (2004).
25. Campos, A. H. & Schor, N. Phyllanthus niruri inhibits calcium oxalate endocytosis by renal tubular cells: its role in urolithiasis. Nephron 81, 393–397 (1999).
26. Lotan, Y. & Pearle, M. S. Cost-effectiveness of primary prevention strategies for nephrolithiasis. J. Urol. 186, 550–555 (2011).
27. Lo, C. Y.-Z. et al. Systematic review of pharmacological, complementary and alternative therapies for the prevention of calcium oxalate stones. Asian J. Urol. (2024). doi:10.1016/j.ajur.2024.04.006
28. Hariton, E. & Locascio, J. J. Randomised controlled trials—the gold standard for effectiveness research. BJOG Int. J. Obstet. Gynaecol. 125, 1716 (2018).
29. Richa, Y., Adjani, T., Tyson, M. & Hennessey, D. B. Inadequate evidence: a critical evaluation of herbal remedies for treating kidney stones. Eur. Urol. Open Sci. 67, S28–S29 (2024).
30. Santos, A. R. S. Chá de quebra-pedra (Phyllanthus niruri) na litíase urinária em humanos e ratos. (1990).
31. Ferraro, P. M., Taylor, E. N., Gambaro, G. & Curhan, G. C. Dietary and lifestyle risk factors associated with incident kidney stones in men and women. J. Urol. (2017).
32. Wang, K. et al. Risk factors for kidney stone disease recurrence: A comprehensive meta-analysis. BMC Urol. 22, 62 (2022).
33. Gómez-Emilsson, A. Logarithmic scales of pleasure and pain: Rating, ranking, and comparing peak experiences suggest the existence of long tails for bliss and suffering. Eff. Altruism Forum (2019). At <https://forum.effectivealtruism.org/posts/gtGe8WkeFvqucYLAF/logarithmic-scales-of-pleasure-and-pain-rating-ranking-and>
34. Gómez-Emilsson, A. & Percy, C. The heavy-tailed valence hypothesis: The human capacity for vast variation in pleasure/pain and how to test it. Front. Psychol. 14, (2023).
35. Leighton, J. The tango of ethics: Intuition, rationality and the prevention of suffering. (Imprint Academic, 2023). At <https://www.imprint.co.uk/product/tango/>
36. Parra-Hinojosa, A. Quantifying the global burden of extreme pain from cluster headaches. Eff. Altruism Forum (2024). At <https://forum.effectivealtruism.org/posts/geh2g2nKb7Kkp26ze/quantifying-the-global-burden-of-extreme-pain-from-cluster>
37. Hoseinkhani, A., Amani, F. & Seddigh-Namini, H. H. Evaluation the success rate of extra corporal shock wave lithotripsy (ESWL) in patients with urinary stones. Int. J. Adv. Med. 5, 1192–1196 (2018).
38. Nielsen, T. K. & Jensen, J. B. Efficacy of commercialised extracorporeal shock wave lithotripsy service: a review of 589 renal stones. BMC Urol. 17, 59 (2017).
39. Di Mauro, E. et al. Efficacy and safety of boldine combined with Phyllanthus niruri and Ononis spinosa in medical expulsive therapy for distal ureteral stones with renal colic: A single-center, retrospective cohort study. Medicina (Mex.) 60, 1455 (2024).
40. Stevenson, A. E. The incidence of urolithiasis in cats and dogs, and the influence of diet in formation and prevention of recurrence. (2002). At <https://www.proquest.com/openview/35647fde9b6cc2ef07258266d931e84f/1>
41. Sharun, K. et al. Prevalence of obstructive urolithiasis in domestic animals: An interplay between seasonal predisposition and dietary imbalance. Iraqi J. Vet. Sci. 35, 227–232 (2021).
42. Elton, D. Kidney stone pain as a potential cause area. Eff. Altruism Forum (2022). At <https://forum.effectivealtruism.org/posts/feuSN98AtvhdqEu2w/kidney-stone-pain-as-a-potential-cause-area>
43. Elton, D. C., Turkbey, E. B., Pickhardt, P. J. & Summers, R. M. A deep learning system for automated kidney stone detection and volumetric segmentation on noncontrast CT scans. Medical Physics 49, 2545–2554 (2022).
Cite as
Gómez-Emilsson, A. & Parra-Hinojosa, A. (2025, February 18). The Quest for a Stone-Free World: Chanca Piedra (Phyllanthus niruri) as an Acute and Prophylactic Treatment for Kidney Stones and Their Associated Extreme Negative Valence. Effective Altruism Forum. https://forum.effectivealtruism.org/posts/JNNrkeWdTHrS87opd/the-quest-for-a-stone-free-world-chanca-piedra-phyllanthus
- ^
While estimating this fraction is outside the scope of this article, we note that the pain one endures is so extreme that it often ranks above childbirth [1]. For a helpful analogy to get a sense of how large this problem is, see the “A Thought Experiment” section.
- ^
We were very surprised with the rate of side effects of melatonin and ashwagandha. Andrés has used these supplements on and off over the years, and he did indeed notice some side effects, but he never thought they would be significant enough to cause so many people to complain about them in these reviews.
- ^
We included reviews of melatonin and ashwagandha partly to see if an “anti-pharmaceutical” and pro–natural-supplements bias could explain the difference between chanca piedra and prescription medicines for kidney stones. We believe that if there is a bias, it is unlikely to be strong enough to explain the reviews of chanca piedra. “Natural” does not seem to inhibit people from sharing particularly negative reactions.
- ^
We also suspect that microdosed flumazenil for benzodiazepine dependence and generalized anxiety disorder is a promising lead in this area. The same goes for frequency-specific microcurrent stimulation, which we believe is studied far less than warranted. More on this in future articles.
- ^
See also OPIS’ work on legalizing access to psilocybin for cluster headache patients.
- ^
Note that one of the largest Facebook groups for kidney stones is called “Kidney Stone Warriors - Worst Pain Ever”.
- ^
Here is one such account: “Help! Long story short[,] had surgery to remove a stone that was blocking my tube. They put a stent in. Removed it at home 6 days ago. 2 hours after removal I'm hit with excruciating pain. 10/10 pain for almost 8 hours straight. This continues for a few days and happens on and off constantly. Until the following Friday where I have 12/10 pain for hours. I barely made it through the day. Saturday all my spasms last 4 hours and are 7/10 pain. Then Sunday I have one spasm for 20 minutes. Monday they come back full force. 2 hours, 4 hours. And currently 2½ all at 9/10 pain while I'm writing this as well. Doctor said it's spasms and they'll go away. I'm about to go crazy.”
- ^
If the data on vitamin C holds up [16], we are talking about doubling the probability of developing kidney stones each year. I estimate that 1000mg a day of the typical vitamin C supplement would result in about half a second of such suffering per pill consumed in expectation, assuming 10 hours of extreme pain per stone.
- ^
Keep in mind that vitamin C is one of the most widely consumed supplements worldwide, and vitamin C megadosing has been touted as a health-boosting intervention by Linus Pauling, a two-time Nobel Prize winner in chemistry. Apparently, Pauling is in denial about the likely role of vitamin C megadosing in increasing kidney stone risk (see his response to being asked if vitamin C causes calcium oxalate stones: “Pauling, a two-time Nobel Prize winner, had for years taken 20,000 milligrams (mgs) of vitamin C daily. He said at the time: ‘Not a single case had been reported in medical literature. But some people who had a tendency to form oxalate stones might do so while taking large amounts of vitamin C, or those with a rare genetic problem.’”)
- ^
Drinking lots of water is one of the top recommendations to avoid kidney stones. However, the difference between drinking 1.5 liters a day and 3.1 liters a day is a reduction of only about 26% in yearly relative risk [18].
- ^
For example, healthline.com suggests avoiding coffee due to its high oxalate content. However, studies actually suggest that coffee has a causal effect in reducing the risk of kidney stones [19,20].
- ^
Keep in mind that these reviews are typically written by people who either had or have kidney stones, so they are already more prone to getting kidney stones than average. This means that, if a typical dose helps so many of them, smaller doses might be enough for the general population, especially for prevention.
- ^
This is also a reason to expect some synergy between chanca piedra and lithotripsy.
- ^
Of course, we are glossing over huge technical caveats. The actual physics of kidney stone formation is an active area of research, and the reasoning presented here may ultimately not work out in practice. That said, it stands to logic and reason that yearly chanca piedra consumption might keep you at a low-enough level of stone deposits that such a protocol will nonetheless prevent stones long-term (even if not via the surface-area–advantage and nucleation elimination argument). See also “How do stones form? Is unification of theories on stone formation possible?” [23]. Moreso, since kidney stones are often spiky, they probably have a certain fractal dimension, which makes the argument of “surface area relative to volume going down as the stones increase” a little weaker. We still think it is likely to hold, but just not as much as if all these stones were perfectly round (then again, if they were perfectly round, they would probably be a lot less painful to pass).
- ^
It is worth noting that most studies we found (including all but the Micali et al. study in the two previous subsections) looking at the efficacy of chanca piedra were carried out at the University of Sao Paulo in Brazil. Brazil has a long history of traditional use of chanca piedra, which is also native to the region. However, none of the papers reported conflicts of interest with the chanca piedra industry.
- ^
The recommendations by the AUA and EAU usually come with a few caveats about when exactly the recommendations apply, so please consult the full guidelines for more details.
- ^
Lotan & Pearle [26] estimated that, in 2011, about 55% of symptomatic kidney stone patients require surgical intervention annually, with half undergoing SWL and half treated with ureteroscopy.
- ^
A cursory look at the reviews suggests that these two products may be comparable to chanca piedra in terms of effectiveness and side-effect profiles. Phosfood seems to be used much more for gallbladder stones, though. Importantly, the way we found about these products was, again, not via search engines or literature searches, but by reading user fora (in particular the Facebook group “kidney stone support group”).
- ^
Notably, they also state: “Despite advancements in the understanding of stone formation, accepted recommendations for preventive therapy have largely remained unchanged for years, and recently, staples of treatment such as thiazides have been challenged.”
- ^
- ^
A clear example of how this problem becomes exacerbated can be found in “Inadequate Evidence: A Critical Evaluation of Herbal Remedies for Treating Kidney Stones” by Richa et al. [29], who concluded that: “There are multiple products available on the internet that claim to prevent or dissolve kidney stones. Only three studies report the use of Phyllanthus niruri, and these are of low quality. No other product is assessed clinically. Based on the findings in this study, urologists should tell their patients to avoid these products.”
- ^
However, patent protection could possibly be obtained for other chanca piedra-related innovations, such as new extraction methods, alternative synthetic versions, specific formulations containing chanca piedra, or new delivery methods.
- ^
If you are interested in additional statistical analyses not included in the dashboard, let us know and we can try to run them. Other footnotes mention all the dimensions we captured for each dataset.
- ^
WebMD classification dimensions: overall rating, effectiveness, ease of use, satisfaction, upvotes/downvotes, reviewer’s age, helps with kidney stones, helps with gallstones, suffers from condition >1 year, makes large amounts of stones (>10), asserts significant pain reduction, provides detailed background, works as a prophylactic, mentions breaking/shrinking/softening/dissolution of stones, mentions quick stone expulsion (≤3 days), deferences (i.e., works better/worse than X), medical personnel was surprised or skeptical, significant pain relief within a day, significant pain relief within a week, consumption method, dose, stone characteristics, provides contact info, admits review sounds incredible, mentions stone passed with no or little pain, provides objective measurements, promotes specific brand, speaks for someone else, side effects, is a super high-quality review, is too good to be true, and any unexpected positive side effects.
- ^
One slightly concerning observation from this analysis is that the homeopathic remedy Oscillococcinum ranked 8th place with 4.5 stars. One possible explanation is that, since Oscillococcinum is intended to treat cold and flu symptoms, it is much more susceptible to placebo effects than treatments for severe pain. It also likely has few side effects given its extreme dilution, assuming no other harmful chemicals are added to the preparation (as a spokesperson put it, "Of course it is safe. There's nothing in it.").
- ^
Two chanca piedra products had ~1k reviews explicitly mentioning “stone”. However, Amazon displays 100 reviews at most for any given filter (e.g., “1-star reviews only”), so we couldn’t scrape all reviews. For example, if one product has 200 1-star reviews, 50 2-star reviews, 50 3-star reviews, 50 4-star reviews, and 800 5-star reviews, one can only view at most 100 of each (so 100, 50, 50, 50, 100), which causes 1-star reviews to be overrepresented (and 5-star reviews to be underrepresented). This only happened for chanca piedra. We adjusted for this bias in the statistics.
- ^
Amazon classification dimensions: stars, helpful upvotes, helps with kidney stones, helps with gallstones, suffers from condition >1 year, makes large amounts of stones (>10), asserts significant pain reduction, works as a prophylactic, mentions breaking/shrinking/softening/dissolution of stones, mentions quick stone expulsion (≤3 days), deferences (i.e., works better/worse than X), medical personnel was surprised or skeptical, significant pain relief within 24 hours, significant pain relief within a week, consumption method, dose, stone characteristics, provides contact info, admits review sounds incredible, mentions stone passed with no or little pain, provides objective measurements, promotes specific brand, speaks for someone else, side effects, is a super high-quality review, is too good to be true, and any unexpected positive side effects.
- ^
We also included alternative names (e.g., “hydroxycitric acid” for garcinia or “tamsulosin” for Flomax) and common misspellings (e.g., “chanka piedra” or “Flowmax”).
- ^
Reddit classification dimensions: Score (upvotes minus downvotes), helps overall with kidney stones, helps with gallstones, suffers from condition >1 year, makes large amounts of stones (>10), asserts significant pain reduction, works as a prophylactic, mentions breaking/shrinking/softening/dissolution of stones, mentions quick stone expulsion (≤3 days), mentions stone passed with no or little pain, side effects, and is a super high-quality review.
- ^
As an additional data point, of the five people who took chanca piedra as per Andrés’ suggestion, none have reported any side effects at all.
- ^
Granted, melatonin is likely not used properly by many users who, for instance, might be taking too much. But just as the proper use of melatonin could reduce side effects, the same would apply to chanca piedra if more research went into how to take it optimally (e.g., in combination with other treatments, as discussed below).
- ^
The review: “Been using Chanca Piedra for over a decade - works great preventing Kidney Stones or getting rid of them quickly when they pop up. However, one thing I have noticed that maybe no one has ever studied. I have definitely been diagnosed with Meiere's Disease - Never ending Tinnitus and bouts of dizziness. My ENT and my Therapist pretty much diagnosed the dizziness to loose ear crystals. Ear crystals are chemically similar to kidney stones, so I suspect the Chanca Piedra may be related to that. Even so, I would rather have recurring bouts of dizziness than kidney stones.”
- ^
Someone we know is particularly concerned about this happening to them. One could take certain precautions, such as understanding the risk factors for kidney stones. For example, Ferraro et al. [31] found that low fluid intake (26% increased risk), higher BMI (14-22% increased risk), and poor adherence to a DASH-style diet (17-20% increased risk) were the strongest modifiable risk factors for developing kidney stones (incidence). The largest risk factors for kidney stone recurrence according to a meta-analysis by Wang et al. [32] are a surgical history of stones (218% higher risk), a history of stones (43% higher risk), being Caucasian (34% higher risk), a family history of stones (19% higher risk), and hypertension (13% higher risk). However, one should also consider the counterfactual: If the person indeed has stones lodged in their kidneys, perhaps sooner or later they will cause issues, and possibly to a more severe degree since the stones might continue to grow.
- ^
In their model, the main driver of cost of no prevention was the cost of surgery, with a point estimate of $6,000 per surgery, since about 55% of cases require surgery.
- ^
See also [35] for further metrics to better quantify extreme suffering, as well as [36] for a case study applying such metrics to the problem of cluster headaches.
- ^
Or its low sodium equivalent to prevent stone formation.
- ^
In the kidney stones support groups we’ve frequented, we often see people complaining that the pain got worse after lithotripsy. They also complain, often, that the doctors they talked to acted like lithotripsy would take care of all the pain and all of the stones.
- ^
We found a handful of reports of people using chanca piedra to treat their pets’ kidney stones. However, a cursory search of the literature did not return many results looking at the incidence of kidney stones among animals. See [40] for cats and dogs in particular (prevalence numbers ranging from 0.25%–1% in some countries) and possibly [41] for further discussions on other domestic animals.
- ^
If you plan to do so, we recommend brands where the product has been tested for purity and includes no other ingredients. For instance, two of the most popular brands on Amazon (Peruvian Naturals and NaturalisimoLife) recently added a label mentioning that the product “might expose you to lead”.
- ^
Alfredo thanks Polaris Ventures in particular for financial support.
I think it'd be better to title this "the quest for a kidney-stone free world". Keeping the words "kidney stone" till late in a long title means that people just browsing the forum front page don't see it, and so can't tell what the post is about. This is really substantial-looking work, and it'd be a shame if it got less clicks than it deserves.
Went in to reading this with a lot of skepticism because RCTs exist for a reason (anecdotal experiences are heavily prone to bias, so they’re not good for determining effectiveness or side effect profiles)
I was disappointed. You justify this analysis of Reddit and Amazon reviews by saying:
This is a fair point but then at the end you don’t just recommend high quality trials but you encourage people to take Chanca piedra without them. So rather than really thinking of this as a bootstrap to trials you’ve actually just bypassed trials and are now recommending a herbal supplement based on Reddit and Amazon comments.
Feels like a Chesterton’s fence situation where you’ve forgotten why RCTs are not just nice but necessary to determine effectiveness and side effect profiles.
Thank you for your feedback, Henry! :)
We'd absolutely love there to be RCTs and definitely encourage larger studies to be run (as mentioned in the Final Recommendations section). It seems like such low-hanging fruit. And one of the main motivations behind this project is that it becomes exactly that incentive needed to get those studies running.
At the same time, it could be years until a large RCT is run. Given the rising incidence of kidney stones worldwide, it seems like asking people to drink more water and eat low-oxalate foods isn't cutting it.
We wrote "Cautiously consider taking chanca piedra yourself" as our very last recommendation. We wanted to strike a balance between recommending something for which large RCTs are still missing and acknowledging that the suffering involved can be so severe that some action could be warranted (especially given that, as we emphasize, chanca piedra seems to cause fewer side effects than e.g. melatonin and ashwagandha).
Very interesting work! A few questions:
I’ll certainly add some chanca piedra to my digital shopping cart and consider actually buying some. I appreciate you taking all the time and effort to do this. I imagine it took a lot of effort.
Thanks for your questions, Joseph!
We've also been wondering about that. I drink a lot of water myself but I tend to forget how much of a hassle it can be for a lot of people who are not used to drinking much water. Other conditions face similar trade-offs. For example, experts might insist that exercising 30 minutes per day is among the most helpful interventions against depression, yet many people would understandably much rather take a pill. The same goes for weight loss or other interventions that require lifestyle changes. Urologists have been recommending increasing water intake for decades, yet incidence keeps growing. Intuitively, it feels more tractable to test the effectiveness of chanca piedra through a large RCT and (if it works) have urologists adopt it as part of their standard recommendations than running global awareness campaigns to drink more water. But I admit I haven't done a BOTEC.
Not yet! But, as part of our next steps, we plan to use this writeup to reach out to experts.
We haven't looked into the distribution in detail (and there's not much data, unfortunately), but we currently think that the median case is likely still very painful. For example, the American Urological Association states:
In this survey, the mean (!) score of kidney stone pain (6.9/10, n=239) was only slightly lower than that of labor pain (7.2/10, n=308) with similar error bars. I think that this is more consistent with a story of the median stone being very painful (than with a story where, say, most stones are only mildly painful). In this (much smaller) survey, 9/93 people mentioned kidney stones to be among their top 3 most painful experiences ever, in line with the ~10% lifetime prevalence. "In other words, there is reason to believe that a large fraction of the people who have had [kidney stones] will rate them as one of their top 3 most painful experiences." Neither of these two surveys selected for e.g. patients seeking medical treatment for stones (as is usually the case in the kidney stone literature).
It's also worth keeping in mind that people who get kidney stones (including small, asymptomatic ones) are at a higher risk of getting stones later on.
I hope this helps! :)
Have you guys thought about what the optimal dosing protocol might be based on current research for use as a prophylactic? Daily for one month per year?
Really cool post, thanks!
Thanks, Hasan! :)
Obviously I want to be cautious about making such a recommendation. 😅 But I'm confident enough in our data (pointing at chanca piedra being safer than e.g. melatonin) that I myself take 500mg once a week, but mostly because (a) that was the default recommended dosage on the bottle I got, and (b) I thought taking it daily would be an overkill given that I think I'm at very low risk. But I could see the rationale for taking it daily for one month per year, as you suggest. Or maybe doing both?
Executive summary: Chanca piedra (Phyllanthus niruri) shows strong potential as both an acute and preventative treatment for kidney stones, with promising anecdotal and preliminary clinical evidence suggesting it may reduce stone formation and alleviate symptoms with minimal side effects.
Key points:
This comment was auto-generated by the EA Forum Team. Feel free to point out issues with this summary by replying to the comment, and contact us if you have feedback.